


 Sign Out
Sign Out

The most common (≥5%) adverse drug reactions (ADRs) reported in patients treated with Phesgo or intravenous pertuzumab in combination with trastuzumab were diarrhea, injection site reaction, infusion-related reactions, asthenia, fatigue, rash, ejection fraction decreased, and anemia.
The most common (≥1%) serious adverse events (SAEs) reported in patients treated with Phesgo or intravenous pertuzumab in combination with trastuzumab were febrile neutropenia, pyrexia, neutropenia, neutropenic sepsis, infusion-related reaction and neutrophil count decreased. SAEs were equally distributed between the Phesgo treatment arm and the intravenous pertuzumab in combination with trastuzumab treatment arm. The following adverse drug reactions were reported with a higher frequency (≥5%) with Phesgo compared to intravenous pertuzumab in combination with trastuzumab: Alopecia 77% vs 70.2%, Dyspnea 10.1% vs 4.4%, and Fatigue 27.8% vs 22.6%.
Tabulated list of adverse drug reactions: The safety profile of Phesgo was overall consistent to the known safety profile of intravenous pertuzumab in combination with trastuzumab and chemotherapy as seen in the pertuzumab and trastuzumab-treated arms of the following pivotal studies (n=3344): CLEOPATRA, in which pertuzumab was given in combination with trastuzumab and docetaxel to patients with MBC (n=453); NEOSPHERE (n=309) and TRYPHAENA (n=218), in which neoadjuvant pertuzumab was given in combination with trastuzumab and chemotherapy to patients with locally advanced, inflammatory or EBC; APHINITY, in which adjuvant pertuzumab was given in combination with trastuzumab and anthracycline-based or non-anthracycline-based, taxane-containing chemotherapy to patients with EBC (n=2364).
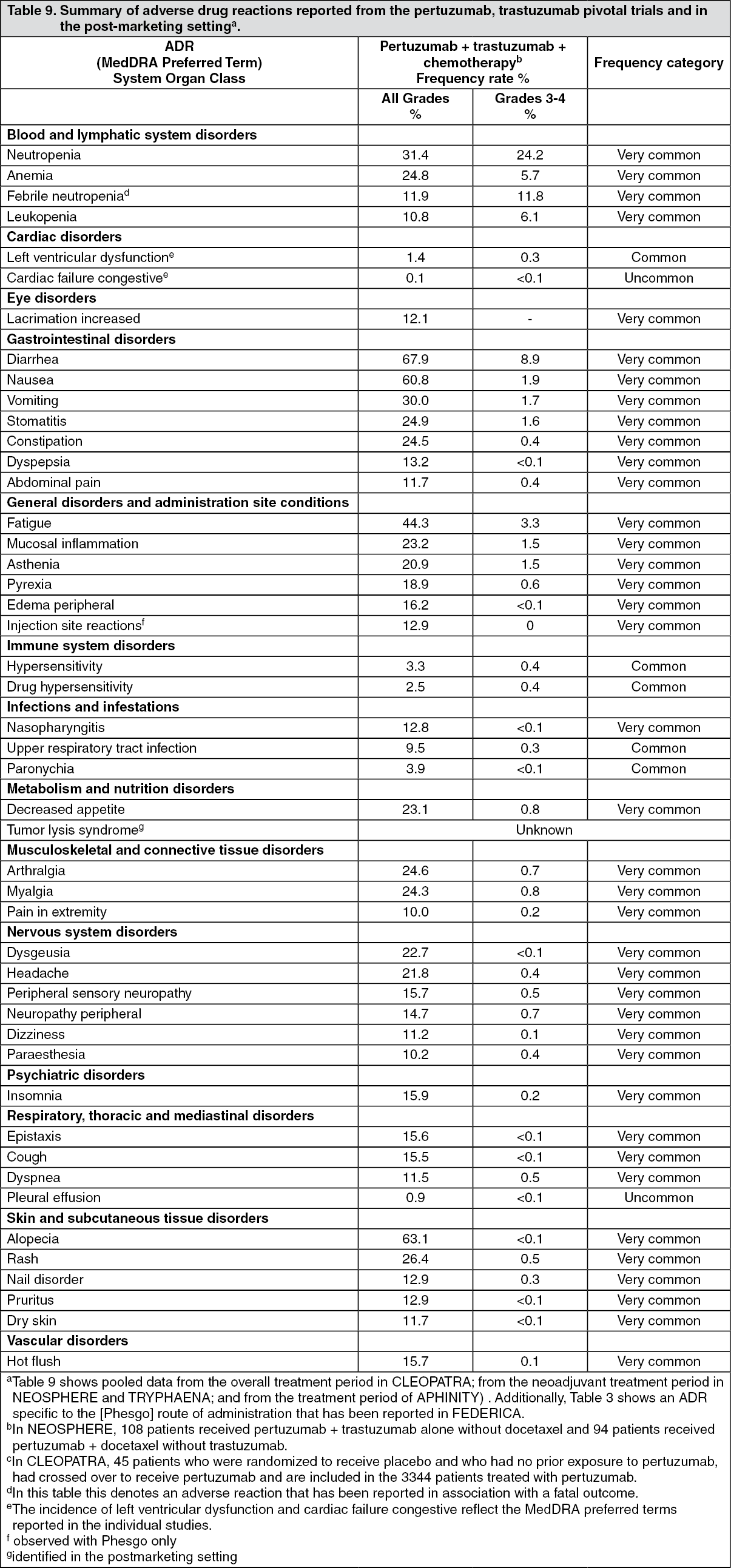
Table 9 presents ADRs that have been reported in association with the use of pertuzumab, trastuzumab and chemotherapy in the pivotal clinical trials and in the post-marketing setting.
As pertuzumab and trastuzumab is used in combination with chemotherapy, it is difficult to ascertain the causal relationship of an adverse reaction to a particular drug.
In this section, the following categories of frequency have been used: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), and unknown (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse drug reactions from clinical trials: Phesgo: Left ventricular dysfunction: In FEDERICA, the incidence of symptomatic heart failure (NYHA class III or IV) with a LVEF decline of at least 10%-points from baseline and to <50% was 0.4% of Phesgo treated patients vs 0% of intravenous pertuzumab and trastuzumab-treated patients. Of the patients who experienced symptomatic heart failure, all Phesgo-treated patients had recovered (defined as 2 consecutive LVEF measurements above 50%) at the data cutoff. Asymptomatic or mildly symptomatic (NYHA class II) declines in LVEF of at least 10%-points from baseline and to <50% (confirmed by secondary LVEF) were reported in 0.4% of Phesgo-treated patients and 0.8% of intravenous pertuzumab and trastuzumab-treated patients, of whom none of the Phesgo-treated patients or intravenous pertuzumab and trastuzumab-treated patients had recovered at the data cutoff.
Injection/infusion-related Reactions: In FEDERICA, an injection/infusion-related reaction was defined as any systemic reaction reported within 24hrs of Phesgo or intravenous pertuzumab in combination with trastuzumab administration. Injection-related reactions were reported in 1.2% of Phesgo-treated patients and infusion-related reactions were reported in 10.3% of intravenous pertuzumab and trastuzumab-treated patients.
Injection site reactions (defined as any local reaction reported within 24 hours of Phesgo) were reported in 12.9% of Phesgo treated patients and were all grade 1 or 2 events.
Hypersensitivity reactions/anaphylaxis: In FEDERICA, the overall frequency of hypersensitivity/anaphylaxis reported events related to HER2- targeted therapy was 1.6% in both the Phesgo-treated patients and intravenous pertuzumab and trastuzumab-treated patients, of which none were NCI-CTCAE (version 4) Grade 3-4 (see Precautions).
Laboratory Abnormalities: In FEDERICA, the incidence of NCI-CTCAE Grade 3-4 decreases in neutrophil counts were balanced in the Phesgo and intravenous pertuzumab and trastuzumab groups.
Intravenous Pertuzumab and Trastuzumab: Left ventricular dysfunction: In CLEOPATRA, the incidence of LVD during study treatment was higher in the placebo-treated group than the pertuzumab-treated group (8.6% and 6.6%, respectively). The incidence of symptomatic LVD was also lower in the pertuzumab-treated group (1.8% in the placebo-treated group vs. 1.5% in the pertuzumab-treated group) (see Precautions).
In NEOSPHERE, in which patients received four cycles of pertuzumab as neoadjuvant treatment, the incidence of LVD (during the overall treatment period) was higher in the pertuzumab, trastuzumab and docetaxel-treated group (7.5%) compared to the trastuzumab and docetaxel-treated group (1.9%). There was one case of symptomatic LVD in the pertuzumab and trastuzumab-treated group.
In TRYPHAENA, the incidence of LVD (during the overall treatment period) was 8.3% in the group treated with pertuzumab plus trastuzumab and 5-fluorouracil, epirubicin and cyclophosphamide (FEC) followed by pertuzumab plus trastuzumab and docetaxel; 9.3% in the group treated with pertuzumab plus trastuzumab and docetaxel following FEC; and 6.6% in the group treated with pertuzumab in combination with TCH. The incidence of symptomatic LVD (congestive heart failure) was 1.3% in the group treated with pertuzumab plus trastuzumab and docetaxel following FEC (this excludes a patient that experienced symptomatic LVD during FEC treatment prior to receiving pertuzumab plus trastuzumab and docetaxel) and also 1.3% in the group treated with pertuzumab in combination with TCH. No patients in the group treated with pertuzumab plus trastuzumab and FEC followed by pertuzumab plus trastuzumab and docetaxel experienced symptomatic LVD.
In the neoadjuvant period of the BERENICE trial, the incidence of NYHA Class III/IV symptomatic LVD (congestive heart failure according to NCI-CTCAE v.4) was 1.5% in the group treated with dose dense AC followed by pertuzumab plus trastuzumab and paclitaxel and none of the patients (0%) experienced symptomatic LVD in the group treated with FEC followed by pertuzumab in combination with trastuzumab and docetaxel. The incidence of asymptomatic LVD (PT ejection fraction decrease according to NCICTCAE v.4) was 7% in the group treated with dose dense AC followed by pertuzumab plus trastuzumab and paclitaxel and 3.5% in the group treated with FEC followed by pertuzumab plus trastuzumab and docetaxel.
In APHINITY, the incidence of symptomatic heart failure (NYHA class III or IV) with a LVEF decline of at least 10%-points from baseline and to <50% was <1% (0.6% of pertuzumab-treated patients vs 0.2% of placebo-treated patients). Of the patients who experienced symptomatic heart failure, 46.7% of pertuzumab-treated patients and 66.7% of placebo-treated patients had recovered (defined as 2 consecutive LVEF measurements above 50%) at the data cutoff. The majority of the events were reported in anthracycline-treated patients. Asymptomatic or mildly symptomatic (NYHA class II) declines in LVEF of at least 10%- points from baseline and to <50% were reported in 2.7% of pertuzumab-treated patients and 2.8% of placebo-treated patients, of whom 79.7% of pertuzumab-treated patients and 80.6% of placebo-treated patients had recovered at the data cutoff.
Infusion-related reaction: An infusion-related reaction was defined in the pivotal trials as any event reported as hypersensitivity, anaphylactic reaction, acute infusion reaction or cytokine release syndrome occurring during an infusion or on the same day as the infusion. In CLEOPATRA, the initial dose of pertuzumab was given the day before trastuzumab and docetaxel to allow for the examination of pertuzumab associated reactions. On the first day when only pertuzumab was administered, the overall frequency of infusion-related reactions was 9.8% in the placebo-treated group and 13.2% in the pertuzumab-treated group, with the majority of reactions being mild or moderate. The most common infusion-related reactions (≥1.0%) in the pertuzumab-treated group were pyrexia, chills, fatigue, headache, asthenia, hypersensitivity, and vomiting.
During the second cycle when all drugs were administered on the same day, the most common infusion related reactions (≥1.0%) in the pertuzumab-treated group were fatigue, drug hypersensitivity, dysgeusia, hypersensitivity, myalgia, and vomiting (see Precautions).
In neoadjuvant and adjuvant trials, pertuzumab was administered on the same day as the other study treatment drugs. Infusion-related reactions occurred in 18.6% -25.0% of patients on the first day of pertuzumab administration (in combination with trastuzumab and chemotherapy). The type and severity of events were consistent with those observed in CLEOPATRA, with a majority of reactions being mild or moderate.
Hypersensitivity/anaphylaxis: In CLEOPATRA, the overall frequency of hypersensitivity/anaphylaxis reported events was 9.3% in the placebo-treated patients and 11.3% in the pertuzumab-treated patients, of which 2.5% and 2.0% were NCI-CTCAE (version 3) grade 3-4, respectively. Overall, 2 patients in placebo-treated group and 4 patients in the pertuzumab-treated group experienced anaphylaxis (see Precautions).
Overall, the majority of hypersensitivity reactions was mild or moderate in severity and resolved upon treatment. Based on modifications made to study treatment, most reactions were assessed as secondary to docetaxel infusions.
In neoadjuvant and adjuvant trials, hypersensitivity/anaphylaxis events were consistent with those observed in CLEOPATRA. In NEOSPHERE, two patients in the pertuzumab and docetaxel-treated group experienced anaphylaxis. In both TRYPHAENA and APHINITY, the overall frequency of hypersensitivity/anaphylaxis was highest in the pertuzumab and TCH treated group (13.2% and 7.6% respectively), of which 2.6% and 1.3% of events, respectively were NCI-CTCAE Grade 3-4.
Laboratory Abnormalities: In the pivotal trials CLEOPATRA, NEOSPHERE, and APHINITY the incidence of NCI-CTCAE Grade 3-4 decreases in neutrophil counts were balanced in the pertuzumab-treated and control groups.
Post marketing experience: Not applicable.
View ADR Monitoring Form