Pharmacology: Pharmacodynamics: Mechanism of action: Pertuzumab and trastuzumab are recombinant humanized immunoglobulin (Ig)G1κ monoclonal antibodies, which target the human epidermal growth factor receptor 2 (HER2, also known as c-erbB-2), a transmembrane glycoprotein with intrinsic tyrosine kinase activity. Pertuzumab and trastuzumab bind to distinct HER2 epitopes, subdomains II and IV, respectively, without competing and have complementary mechanisms for disrupting HER2 signaling. This results in augmented anti-proliferative activity in vitro and in vivo when pertuzumab and trastuzumab are given in combination.
Additionally, the Fc portion of both their IgG1 framework provides for potent activation of antibody-dependent cell-mediated cytotoxicity (ADCC). In vitro, both pertuzumab and trastuzumab ADCC are exerted preferentially on HER2-overexpressing cancer cells compared with cancer cells that do not overexpress HER2.
Clinical/efficacy studies: This section presents the clinical experience from Phesgo and intravenous pertuzumab in combination with trastuzumab patients with HER2-positive early and metastatic breast cancer. HER2 overexpression in all trials outlined as follows was determined at a central laboratory and defined as a score of 3+ by IHC or an ISH amplification ratio ≥2.0.
Early Breast Cancer: Fixed-dose combination of pertuzumab and trastuzumab Phesgo: FEDERICA WO40324: FEDERICA is an open-label, multicenter, randomized study conducted in 500 patients with HER2-positive early breast cancer that is operable or locally advanced (including inflammatory) breast cancer with a tumor size >2 cm or node-positive in the neoadjuvant and adjuvant setting. Patients were randomized to receive 8 cycles of neoadjuvant chemotherapy with concurrent administration of 4 cycles of either Phesgo or intravenous pertuzumab and trastuzumab during cycles 5-8. Investigators selected one of two of the following neoadjuvant chemotherapy regimens for individual patients: 4 cycles of doxorubicin (60 mg/m
2) and cyclophosphamide (600 mg/m
2) every 2 weeks followed by paclitaxel (80 mg/m
2) weekly for 12 weeks; 4 cycles of doxorubicin (60 mg/m
2) and cyclophosphamide (600 mg/m
2) every 3 weeks followed by 4 cycles of docetaxel (75 mg/m
2 for the first cycle and then 100 mg/m
2 at subsequent cycles at the investigator's discretion) every 3 weeks.
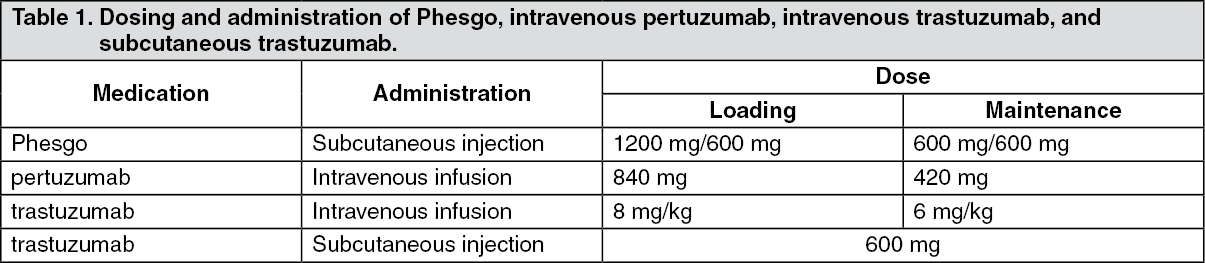
Following surgery, patients continued therapy with Phesgo or intravenous pertuzumab and trastuzumab as treated prior to surgery, for an additional 14 cycles, to complete 18 cycles of HER2-targeted therapy. Patients also received adjuvant radiotherapy and endocrine therapy as per local practice. In the adjuvant setting, substitution of intravenous trastuzumab for subcutaneous trastuzumab SC was permitted at investigator discretion. HER2-targeted therapy was administered every 3 weeks according to Table 1 as follows: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
FEDERICA was designed to demonstrate non-inferiority of the pertuzumab Cycle 7 (i.e., pre-dose Cycle 8) serum C
trough of pertuzumab within Phesgo compared with intravenous pertuzumab (primary endpoint). Additional secondary endpoints included non-inferiority of the Cycle 7 serum trastuzumab C
trough of trastuzumab within Phesgo compared with intravenous trastuzumab, efficacy [total pathological complete response (tpCR)], and safety outcomes. Demographics were well balanced between the two treatment arms and the median age of patients treated in the study was 51 years. The majority of patients had hormone receptor-positive disease (61.2%), node-positive disease (57.6%), and were Caucasian (65.8%).
Non-inferiority of the pertuzumab and trastuzumab exposure from Phesgo was demonstrated (see Pharmacokinetics as follows). The analysis of secondary efficacy endpoint, tpCR, defined as an absence of invasive disease in the breast and axilla (ypT0/is, ypN0), is shown in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
Intraveneous Pertuzumab and Trastuzumab: Neoadjuvant Treatment: NEOSPHERE (WO20697): NEOSPHERE is a multicenter, randomized Phase II clinical trial conducted in 417 patients with operable, locally advanced, or inflammatory HER2-positive breast cancer (T2-4d) who were scheduled for neoadjuvant therapy. Patients were randomized to receive one of four neoadjuvant regimens prior to surgery as follows: trastuzumab plus docetaxel, pertuzumab plus trastuzumab and docetaxel, pertuzumab plus trastuzumab, or pertuzumab plus docetaxel. Randomization was stratified by breast cancer type (operable, locally advanced, or inflammatory) and estrogen (ER) or progesterone (PgR) positivity.
Pertuzumab and trastuzumab were administered intravenously as outlined in Table 1 for 4 cycles. Following surgery all patients received three cycles of 5-Fluorouracil (600 mg/m
2), epirubicin (90 mg/m
2), cyclophosphamide (600 mg/m
2) (FEC) given intravenously every three weeks and trastuzumab administered intravenously every three weeks to complete one year of therapy. Patients in the pertuzumab plus trastuzumab and docetaxel arm received docetaxel every three weeks for four cycles prior to FEC after surgery so that all patients received equivalent cumulative doses of the chemotherapeutic agents and trastuzumab.
The primary endpoint of the study was pathological complete response (pCR) rate in the breast (ypT0/is). Secondary efficacy endpoints were clinical response rate, breast conserving surgery rate (T2-3 only), disease-free survival (DFS), and PFS. Additional exploratory pCR rates included nodal status (ypT0/isN0 and ypT0N0).
Demographics were well balanced [median age was 49-50 years old, the majority were Caucasian (71%)] and all were female. Overall 7% of patients had inflammatory breast cancer, 32% had locally advanced breast cancer and 61% had operable breast cancer. Approximately half the patients in each treatment group had hormone receptor-positive disease (defined as ER positive and/or PgR positive).
The efficacy results are summarized in Table 3. A statistically significant and clinically meaningful improvement in pCR rate (ypT0/is) was observed in patients receiving pertuzumab plus trastuzumab and docetaxel compared to patients receiving trastuzumab and docetaxel (45.8% vs 29.0%, p value = 0.0141). A consistent pattern of results was observed regardless of pCR definition.
Pathological complete response (pCR) rates as well as the magnitude of improvement with pertuzumab were lower in the subgroup of patients with hormone receptor-positive tumors than in patients with hormone receptor-negative tumors (5.9% to 26.0% and 27.3% to 63.2%, respectively).
TRYPHAENA (BO22280): TRYPHAENA is a multicenter, randomized Phase II clinical study conducted in 225 patients with HER2-positive locally advanced, operable, or inflammatory (T2-4d) breast cancer. Patients were randomized to receive one of three neoadjuvant regimens prior to surgery as follows: 3 cycles of FEC followed by 3 cycles of docetaxel all in combination with pertuzumab and trastuzumab, 3 cycles of FEC alone followed by 3 cycles of docetaxel and trastuzumab in combination with pertuzumab, or 6 cycles of TCH in combination with pertuzumab. Randomization was stratified by breast cancer type (operable, locally advanced, or inflammatory) and ER and/or PgR positivity.
Pertuzumab and trastuzumab were administered intravenously as outlined in Table 1. 5-Fluorouracil (500 mg/m
2), epirubicin (100 mg/m
2), cyclophosphamide (600 mg/m
2) were given intravenously every three weeks for 3 cycles. Docetaxel was given as an initial dose of 75 mg/m
2 IV infusion every three weeks with the option to escalate to 100 mg/m
2 at the investigator's discretion if the initial dose was well tolerated. However, in the pertuzumab in combination with TCH arm, docetaxel was given intravenously at 75 mg/m
2 and no escalation was permitted and carboplatin (AUC 6) was given intravenously every three weeks. Following surgery all patients received trastuzumab to complete one year of therapy, which was administered intravenously every 3 weeks.
The primary endpoint of this study was cardiac safety during the neoadjuvant treatment period of the study (see Adverse Reactions). Secondary efficacy endpoints were pCR rate in the breast (ypT0/is), DFS, PFS and OS.
Demographics were well balanced (median age was 49-50 years old, the majority were Caucasian (77%) and all were female. Overall 6% of patients had inflammatory breast cancer, 25% had locally advanced breast cancer and 69% had operable breast cancer, with approximately half the patients in each treatment group had ER-positive and/or PgR-positive disease.
High pCR rates were observed in all 3 treatment arms (see Table 3). A consistent pattern of results was observed regardless of pCR definition. pCR rates were lower in the subgroup of patients with hormone receptor-positive tumors than in patients with hormone receptor-negative tumors (46.2% to 50.0% and 65.0% to 83.8% respectively). (See Table 3.)
Click on icon to see table/diagram/image
BERENICE (WO29217): BERENICE is a non-randomized, open-label, multicenter, multinational, Phase II trial conducted in 401 patients with HER2-positive locally advanced, inflammatory, or early-stage HER2-positive breast cancer.
The BERENICE study included two parallel groups of patients. Patients considered suitable for neoadjuvant treatment with trastuzumab plus anthracycline/taxane-based chemotherapy were allocated to receive one of the two following regimens prior to surgery as follows: Cohort A - 4 cycles of two-weekly doxorubicin and cyclophosphamide (dose dense AC) followed by 4 cycles of pertuzumab in combination with trastuzumab and paclitaxel.
Cohort B - 4 cycles of FEC followed by 4 cycles of pertuzumab in combination with trastuzumab and docetaxel.
Pertuzumab and trastuzumab were administered intravenously as outlined in Table 1. Doxorubicin 60 mg/m
2 IV and cyclophosphamide 600 mg/m
2 IV were administered every 2 weeks (ddAC) for four cycles (Cycles 1-4) with G-CSF (granulocyte colony stimulating factor) support at investigator discretion, followed by paclitaxel 80 mg/m
2 IV weekly for 12 weeks (Cycles 5-8), with pertuzumab and trastuzumab every 3 weeks during Cycles 5-8 (from the start of paclitaxel; four cycles of pertuzumab and trastuzumab in total during the neoadjuvant period). 5-Fluorouracil (500 mg/m
2), epirubicin (100 mg/m
2), cyclophosphamide (600 mg/m
2) were given intravenously every three weeks for 4 cycles. Docetaxel was given at an initial dose of 75 mg/m
2 IV infusion every three weeks with the option to escalate to 100 mg/m
2 at the investigator's discretion if the initial dose was well tolerated. Following surgery all patients received pertuzumab and trastuzumab which were administered intravenously every 3 weeks, to complete one year of therapy.
The primary endpoint of this study was cardiac safety during the neoadjuvant treatment period of the study (see Precautions). Key secondary endpoints at the time of primary analysis were neoadjuvant safety and pCR rate in the breast and nodes (i.e. ypT0/is ypN0). Long-term clinical and safety outcomes will also be assessed (IDFS, EFS and OS, not yet available).
Demographics of the patients were well balanced between the groups. The median age of the patients was 49 years, the majority of patients were Caucasian (83%) and all but one patient was female. Approximately two-thirds of patients (64.3% [n = 128] in Cohort A and 61.7% [n = 124] in Cohort B) had hormone receptor-positive disease.
High pCR rates were observed in both treatment arms, with pCR (ypT0/is ypN0) rates of 61.8% in Cohort A and 60.7% in Cohort B. A consistent pattern of results was observed regardless of pCR definition. pCR rates were lower in the subgroup of patients with hormone receptor-positive tumors than in patients with hormone receptor-negative tumors in both Cohorts (51.6% to 81.5% and 57.3% to 68.0% respectively).
Adjuvant Treatment: APHINITY (BO25126): APHINITY is a multicenter, randomized, double-blind, placebo-controlled Phase III trial conducted in 4804 patients with HER2-positive early breast cancer who had their primary tumor excised prior to randomization. Patients were then randomized to receive pertuzumab or placebo, in combination with adjuvant trastuzumab and chemotherapy. Investigators selected one of the following anthracycline-based or non-anthracycline-based chemotherapy regimens for individual patients: 3 or 4 cycles of FEC or 5-fluorouracil, doxorubicin and cyclophosphamide (FAC), followed by 3 or 4 cycles of docetaxel or 12 cycles of weekly paclitaxel; 4 cycles of AC or EC, followed by 3 or 4 cycles of docetaxel or 12 cycles of weekly paclitaxel; 6 cycles of docetaxel in combination with carboplatin.
Pertuzumab and trastuzumab were administered intravenously as outlined in Table 1 starting on Day 1 of the first taxane-containing cycle, for a total of 52 weeks (maximum 18 cycles) or until recurrence, withdrawal of consent or unmanageable toxicity. Standard doses of 5-fluorouracil, epirubicin, doxorubicin, cyclophosphamide, docetaxel, paclitaxel and carboplatin were administered. After completion of chemotherapy, patients received radiotherapy and/or hormone therapy as per local clinical standard.
The primary endpoint of the study was invasive disease-free survival (IDFS), defined as the time from randomization to first occurrence of ipsilateral local or regional invasive breast cancer recurrence, distant recurrence, contralateral invasive breast cancer, or death from any cause.
Demographics were well balanced between the two treatment arms. The median age was 51 years, and over 99% of patients were female. The majority of patients had node-positive (63%) and/or hormone receptor-positive disease (64%), and were Caucasian (71%).
After a median follow-up to 45.4 months, the APHINITY study demonstrated 19% (hazard ratio [HR] = 0.81) reduction in risk of recurrence or death in patients randomized to receive pertuzumab compared with patients randomized to receive placebo.
The efficacy results from the APHINITY trial are summarized in Table 4 and in Figures 1 and 2. (See Table 4 and Figure 1.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The estimate of IDFS at 4-years was 92.3% in the pertuzumab-treated group versus 90.6% in the placebo-treated group. At the time of the estimate the median follow-up was 45.4 months.
Results of Subgroup Analysis: Consistent results were observed across the majority of pre-specified patient subgroups. The benefits of pertuzumab were more apparent for patients in certain high risk groups, notably patients with node-positive or hormone receptor-negative disease (see Figure 2 as follows).
Click on icon to see table/diagram/image
Estimates of IDFS rates in the node positive subgroup were 92.0% versus 90.2% at 3 years and 89.9% vs. 86.7% at 4 years in pertuzumab-treated patients versus the placebo-treated patients, respectively. In the node negative subgroup estimates of IDFS rates were 97.5% versus 98.4% at 3 years and 96.2% versus 96.7% at 4 years in pertuzumab-treated patients versus placebo-treated patients, respectively.
In the hormone receptor-positive subgroup estimates of IDFS were 94.8% versus 94.4% at 3 years and 93.0% versus 91.6% at 4 years in pertuzumab-treated patients versus placebo-treated patients, respectively. In the hormone receptor-negative subgroup estimates of IDFS rates were 92.8% versus 91.2% at 3 years and 91.0% versus 88.7% at 4 years in pertuzumab-treated patients versus placebo-treated patients, respectively.
Patient Reported Outcomes (PRO): Secondary endpoints included the assessment of patient-reported global health status, role and physical function, and treatment symptoms using the EORTC QLQ-C30 and EORTC QLQ-BR23 questionnaires. In the analyses of patient-reported outcomes, a 10-point difference was considered clinically meaningful.
Patients' physical function, global health status and diarrhea scores showed a clinically meaningful change during chemotherapy in both treatment arms. The mean decrease from baseline at that time for physical function was -10.7 (95% CI-11.4, -10.0) in the pertuzumab-arm and -10.6 (95% -11.4, -9.9) in the placebo arm; global health status was -11.2 (95% CI -12.2, -10.2) in the pertuzumab-arm and -10.2 (95% CI -11.1, -9.2) in the placebo arm. Change in diarrhea symptoms increased to +22.3 (95% CI 21.0, 23.6) in the pertuzumab-arm versus +9.2 (95% CI 8.2, 10.2) in the placebo arm.
Thereafter in both arms, physical function and global health status scores returned to baseline levels during targeted treatment. Diarrhea symptoms returned to baseline after HER2 therapy in the pertuzumab-arm. The addition of pertuzumab to trastuzumab plus chemotherapy did not affect patients' overall role function over the course of the study.
Metastatic Breast Cancer: CLEOPATRA (WO20698): CLEOPATRA is a multicenter, randomized, double-blind, placebo-controlled Phase III clinical trial conducted in 808 patients with HER2-positive metastatic or locally recurrent unresectable breast cancer who have not received previous anti-HER2 therapy or chemotherapy for their metastatic disease. Patients were randomized 1:1 to receive placebo plus trastuzumab and docetaxel (placebo-treated) or pertuzumab plus trastuzumab and docetaxel (pertuzumab-treated). Randomization was stratified by prior treatment status (de novo or prior adjuvant / neoadjuvant therapy) and geographic region (Europe, North America, South America and Asia). Patients with prior adjuvant or neoadjuvant therapy were required to have a disease free interval of at least 12 months before enrolment into the trial.
Pertuzumab and trastuzumab were administered intravenously as outlined in Table 1. Patients were treated with pertuzumab and trastuzumab until disease progression, withdrawal of consent or unmanageable toxicity. Docetaxel was given as an initial dose of 75 mg/m
2 IV infusion every 3 weeks for at least 6 cycles. The dose of docetaxel could be escalated to 100 mg/m
2 at the investigator's discretion if the initial dose was well tolerated. At the time of the primary analysis, the mean number of cycles of study treatment received was 16.2 in the placebo treatment group and 19.9 in the pertuzumab-treated group.
The primary endpoint of the study was progression-free survival (PFS) as assessed by an independent review facility (IRF) and defined as the time from the date of randomization to the date of disease progression or death (from any cause) if the death occurred within 18 weeks of the last tumor assessment. Secondary efficacy endpoints were overall survival (OS), PFS (investigator-assessed), objective response rate (ORR), duration of response, and time to symptom progression according to the FACT B QoL questionnaire.
Demographics were well balanced (median age was 54 years old, the majority were Caucasian (59%) and all were female with the exception of 2 patients). Approximately half the patients in each treatment group had hormone receptor-positive disease (defined as estrogen receptor [ER] positive and/or progesterone receptor [PgR] positive) and approximately half of the patients in each treatment group had received prior adjuvant or neo-adjuvant therapy (192 patients [47.3%] in the placebo-treated group vs 184 patients [45.8%] pertuzumab-treated group). At the time of the primary progression-free survival analysis, a total of 242 patients (59%) in the placebo-treated group and 191 patients (47.5%) in the pertuzumab-treated group had IRF-confirmed progressive disease or had died within 18 weeks of their last tumor assessment.
At the time of the primary analysis the CLEOPATRA study demonstrated a statistically significant improvement in IRF-assessed PFS (hazard ratio [HR] = 0.62, 95% CI = 0.51, 0.75, p<0.0001) in the pertuzumab-treated group compared with the placebo-treated group, and an increase in median PFS of 6.1 months (median PFS of 12.4 months in the placebo-treated group vs 18.5 months in the pertuzumab-treated group) (see Figure 3). The results for investigator-assessed PFS were comparable to those observed for IRF-assessed PFS (median PFS was 12.4 months for placebo vs 18.5 months for pertuzumab) (see Table 5). Consistent results were observed across pre-specified patient subgroups including the subgroups based on stratification factors of geographic region and prior adjuvant /neoadjuvant therapy or de novo metastatic breast cancer (see Figure 4).
The efficacy results from the CLEOPATRA trial are summarized in Table 5 as follows. (See Table 5 and Figures 3 and 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
At the primary analysis of efficacy, an interim analysis of OS showed a strong trend suggestive of a survival benefit in favor of the Perjeta-treated group.
An interim analysis of OS performed one year after the primary analysis of efficacy, demonstrated a statistically significant OS benefit in favor of the pertuzumab-treated group (HR 0.66, p = 0.0008 log-rank test). The median time to death was 37.6 months in the placebo-treated group but had not yet been reached in the pertuzumab-treated group.
The final analysis of OS was performed when 389 patients had died (221 in the placebo-treated group and 168 in the pertuzumab-treated group). The statistically significant OS benefit in favor of the pertuzumab-treated group was maintained (HR 0.68, p = 0.0002 log-rank test). The median time to death was 40.8 months in the placebo-treated group and 56.5 months in the pertuzumab-treated group (see Table 5, Figure 5). (See Figure 5.)
Click on icon to see table/diagram/image
There was no statistically significant difference between treatment groups in Health Related Quality of Life as assessed by time to symptom progression on the FACTB TOI-PFB subscale, defined as a 5 point reduction in subscale score (HR =0.97, 95% CI =0.81; 1.16). In an exploratory analysis, patients treated with pertuzumab in combination with trastuzumab and docetaxel experienced a lower risk of symptom progression on the FACT-B breast cancer subscale (defined as a 2 point reduction in subscale score) compared to those treated with trastuzumab and docetaxel alone (HR =0.78, 95% CI =0.65; 0.94).
Immunogenicity: As with all therapeutic proteins, there is the potential for immune response in patients treated with Phesgo. Immunogenicity assay results are highly dependent on several factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications and underlying disease. For these reasons, comparison of incidence of treatment-emergent antibodies to Phesgo with the incidence of antibodies to other products may be misleading.
In the FEDERICA study, the incidence of treatment-emergent anti-pertuzumab and anti-trastuzumab antibodies was 3% (7/237) and 0.4% (1/237), respectively, in patients treated with intravenous pertuzumab and trastuzumab.
The incidence of treatment-emergent anti-pertuzumab, anti-trastuzumab, and anti- vorhyaluronidase alfa antibodies was 4.8% (11/231), 0.9% (2/232), and 0.9% (2/225), respectively, in patients treated with Phesgo. The clinical relevance of the development of anti-pertuzumab, anti-trastuzumab or anti-vorhyaluronidase alfa antibodies after treatment with Phesgo is unknown.
Pharmacokinetics: Pertuzumab and trastuzumab exposure following subcutaneous administration of Phesgo (1200 mg pertuzumab/600 mg trastuzumab loading dose followed by 600 mg pertuzumab/600 mg trastuzumab every 3 weeks) in the FEDERICA study is shown in Table 1. The pharmacokinetic (PK) results for the primary endpoint of pertuzumab Cycle 7 C
trough (i.e., pre-dose cycle 8), showed non-inferiority of pertuzumab within Phesgo (geometric mean 88.7 mcg/mL) compared to intravenous pertuzumab (geometric mean 72.4 mcg/mL) with a geometric mean ratio of 1.22 (90% CI: 1.14–1.31). The lower boundary of the two-sided 90% confidence interval for the geometric mean ratio of pertuzumab within Phesgo and intravenous pertuzumab was 1.14, i.e., greater than the predefined margin of 0.8.
The PK results for the secondary endpoint, trastuzumab Cycle 7 C
trough (i.e., predose Cycle 8), showed non-inferiority of trastuzumab within Phesgo (geometric mean 58.7 mcg/mL) compared to intravenous trastuzumab (geometric mean 44.1 mcg/mL) with a geometric mean ratio of 1.33 (90% CI: 1.24-1.43).
A population PK model of pertuzumab with linear elimination from the central compartment was constructed using pooled pertuzumab within Phesgo and intravenous pertuzumab PK data from FEDERICA to describe the observed pertuzumab PK concentrations following subcutaneous Phesgo administration and intravenous pertuzumab administration.
A population PK model with parallel linear and nonlinear elimination from the central compartment was constructed using pooled trastuzumab PK data from the phase III study BO22227 (Hannah) of subcutaneous trastuzumab vs. intravenous trastuzumab, to describe the observed PK concentrations following intravenous trastuzumab or subcutaneous trastuzumab administration in HER2 positive EBC patients. The PK analysis using the HANNAH population PK model demonstrated that there was no impact on the PK of trastuzumab within Phesgo from pertuzumab within Phesgo as consistent PK were observed between trastuzumab within Phesgo and subcutaneous trastuzumab.
The population PK predicted pertuzumab and trastuzumab exposures are summarized in Table 6 as follows. (See Table 6.)
Click on icon to see table/diagram/image
Absorption: The median maximum serum concentration (C
max) of pertuzumab within Phesgo and time to maximal concentration (T
max) were 157 ug/mL and 3.82 days, respectively. Based on population PK analysis, the absolute bioavailability was 0.712 and the first-order absorption rate (K
a) is 0.348 (1/day).
The median maximum serum concentration (C
max) of trastuzumab within Phesgo and time to maximal concentration (T
max) were 117 ug/mL and 3.85 days, respectively. Based on population PK analysis, the absolute bioavailability was 0.771 and the first-order absorption rate (K
a) is 0.404 (1/day).
Distribution: Based on population PK analysis, the volume of distribution of the central (Vc) compartment of pertuzumab within Phesgo in the typical patient, was 2.77 L.
Based on population PK analysis, the volume of distribution of the central (Vc) compartment of subcutaneous trastuzumab in the typical patient, was 2.91 L.
Metabolism: The metabolism of Phesgo has not been directly studied. Antibodies are cleared principally by catabolism.
Elimination: Based on population pharmacokinetic (PK) analysis, the clearance of pertuzumab within Phesgo was 0.163 L/day and the elimination half-life (t
½) was approximately 24.3 days.
Based on population pharmacokinetic (PK) analysis, the linear clearance of subcutaneous trastuzumab was 0.111 L/day. Trastuzumab is estimated to reach concentrations that are <1 μg/mL (approximately 3% of the population predicted C
min,ss, or about 97% washout) in at least 95% patients 7 months after the last dose.
Pharmacokinetics in Special Populations: Pediatric Population: No studies have been conducted to investigate the pharmacokinetics of Phesgo in the pediatric population.
Geriatric Population: No studies have been conducted to investigate the pharmacokinetics of Phesgo in geriatric patients.
In population PK analyses of pertuzumab within Phesgo and intravenous pertuzumab, age was not found to significantly affect PK of pertuzumab.
In population PK analyses of subcutaneous or intravenous trastuzumab, age has been shown to have no effect on the disposition of trastuzumab.
Renal impairment: No formal PK study of Phesgo has been conducted in patients with renal impairment.
Based on population PK analyses of pertuzumab within Phesgo and intravenous pertuzumab, renal impairment was shown not to affect pertuzumab exposure; however, only limited data from patients with severe renal impairment were included in population PK analyses.
In a population pharmacokinetic analysis of subcutaneous and intravenous trastuzumab, renal impairment was shown not to affect trastuzumab disposition.
Hepatic impairment: No formal pharmacokinetic study of Phesgo has been conducted in patients with hepatic impairment.
Toxicology: Preclinical Safety Data: No dedicated studies were conducted with the combination of subcutaneous pertuzumab, trastuzumab, and vorhyaluronidase alfa.
Subcutaneous and Intravenous Pertuzumab and Trastuzumab: Subcutaneous pertuzumab (250 mg/kg/week for 4 weeks) and intravenous pertuzumab (up to 150 mg/kg weekly for up to 26 weeks) was well tolerated in cynomolgus monkeys (binding species), except for the development of diarrhea. With intravenous pertuzumab doses of 15 mg/kg and higher, intermittent mild treatment-associated diarrhea was noted. In a subset of monkeys, chronic dosing (26 weekly doses) resulted in episodes of diarrhea-related dehydration which were managed with intravenous fluid replacement therapy. Trastuzumab was well tolerated in mice (non-binding species), rabbits (non-binding species) and Macaque (rhesus and cynomolgus) monkeys (binding species) in single-dose (IV) and repeat-dose toxicity (SC and IV) studies of up to 13 weeks (25 mg/kg twice weekly) or 26 weeks (25 mg/kg weekly) duration, respectively. No evidence of acute or chronic toxicity was identified.
Intravenous trastuzumab: Lactation: A study conducted in cynomolgus monkeys that had received trastuzumab at doses 25 times that of the weekly human maintenance dose of 2 mg/kg intravenous trastuzumab from days 120 to 150 of pregnancy, demonstrated that trastuzumab is secreted in the milk postpartum. The exposure to trastuzumab in utero and the presence of trastuzumab in the serum of these infant monkeys was not associated with any adverse effects on their growth or development from birth to 1 month of age.
Carcinogenicity: No carcinogenicity studies have been performed to establish the carcinogenic potential of pertuzumab or trastuzumab within Phesgo.
Genotoxicity: No studies have not been performed to evaluate the mutagenic potential of pertuzumab or trastuzumab within Phesgo.
Impairment of Fertility: Intravenous Pertuzumab: No specific fertility studies in animals have been performed to evaluate the effect of pertuzumab. No adverse effects on male and female reproductive organs were observed in repeat-dose toxicity studies of up to six month duration in cynomolgus monkeys.
Intravenous Trastuzumab: Reproduction studies of female fertility have been conducted in cynomolgus monkeys at doses up to 25 times that of the weekly human maintenance dose of 2 mg/kg intravenous trastuzumab and have revealed no evidence of impaired fertility. Additionally, no adverse effects on male and female reproductive organs were observed in repeat-dose toxicity studies of up to six month duration in cynomolgus monkeys.
Reproductive toxicity: Intravenous Pertuzumab: Reproductive toxicology studies have been conducted in cynomolgus monkeys at loading doses of 30 to 150 mg/kg and maintenance doses of 10 to 100 mg/kg achieving clinically relevant exposures. Intravenous administration of pertuzumab from Gestation Day (GD) 19 through 50 (period of organogenesis) has been shown to be embryotoxic with a dose dependent increase in embryo-fetal deaths between GD 25 to 70. Delayed renal development and oligohydramnios were identified at GD100.
Intravenous Trastuzumab: Reproduction studies have been conducted in cynomolgus monkeys at doses up to 25 times that of the weekly human maintenance dose of 2 mg/kg intravenous trastuzumab and have revealed no evidence of harm to the fetus. Placental transfer of trastuzumab during the early (days 20 - 50 of gestation) and late (days 120 - 150 of gestation) fetal development period was observed.
Other: Subcutaneous trastuzumab: Subcutaneous trastuzumab with vorhyaluronidase alfa was well tolerated in a rabbit local tolerance study (non-binding species) and in a 13-week repeat dose toxicity study in cynomolgus monkeys (binding species).



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image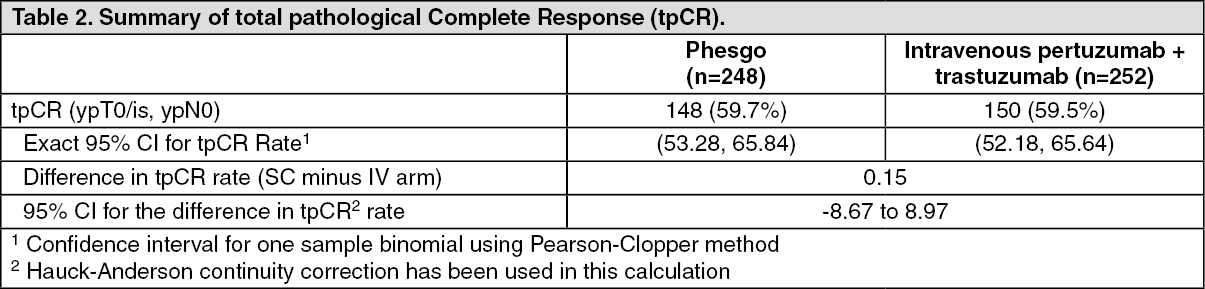 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image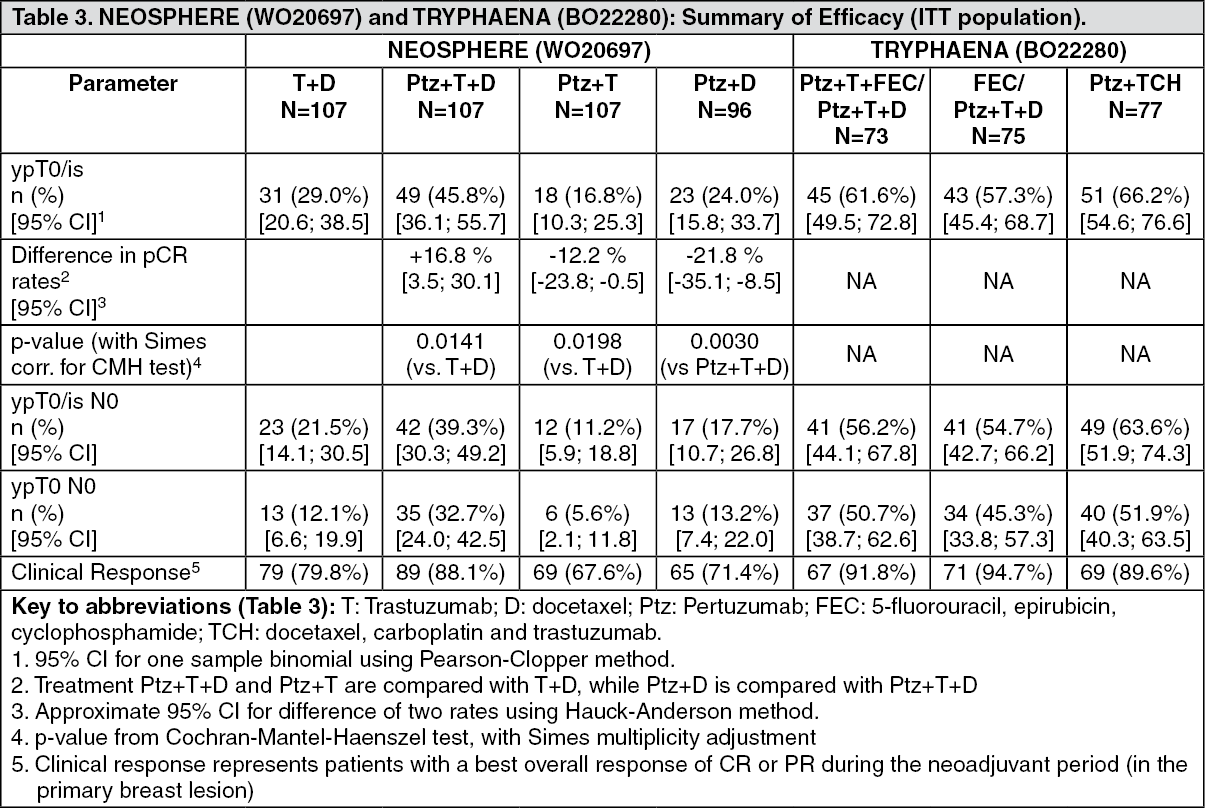 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image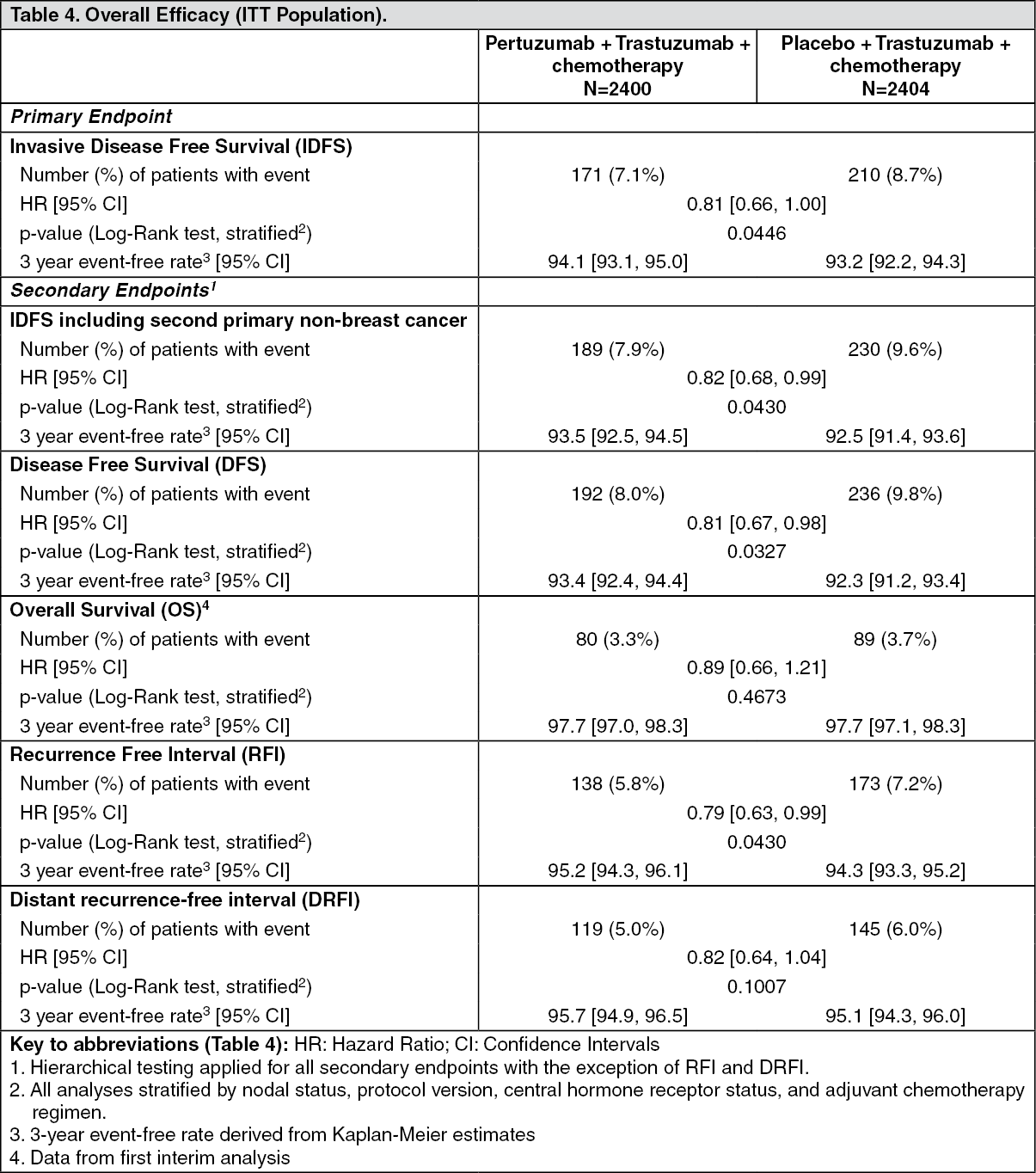 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image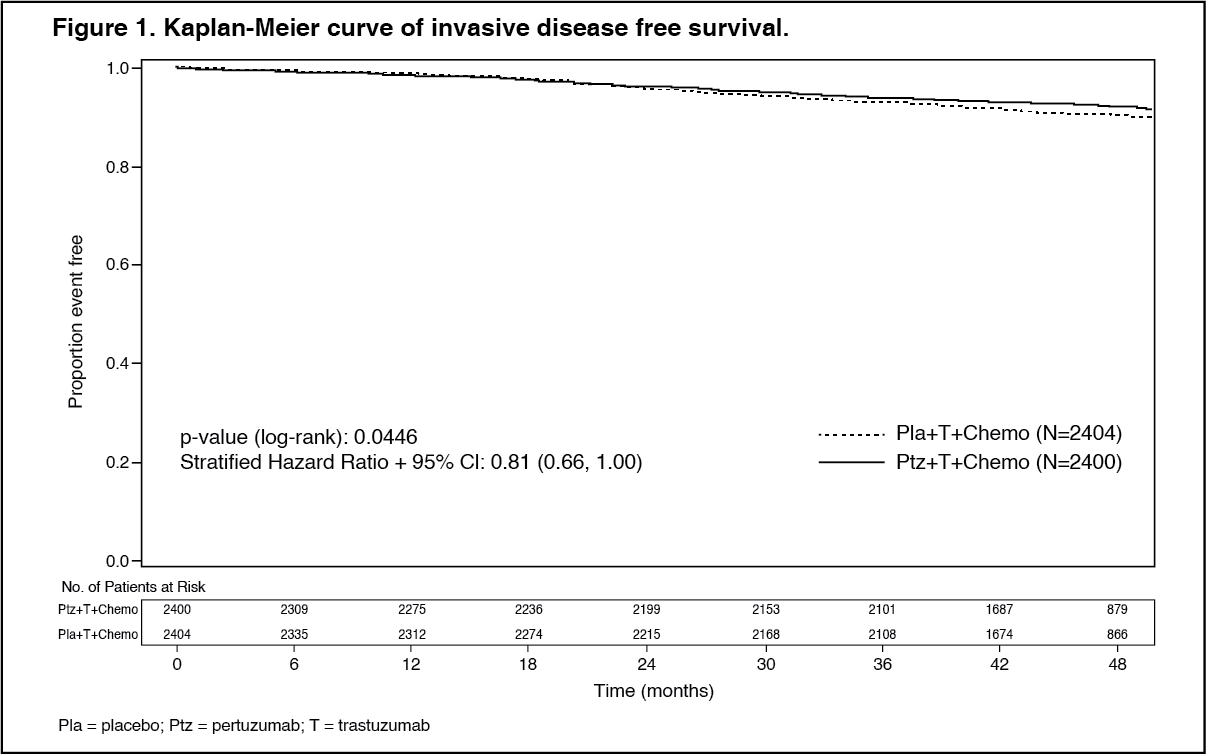 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image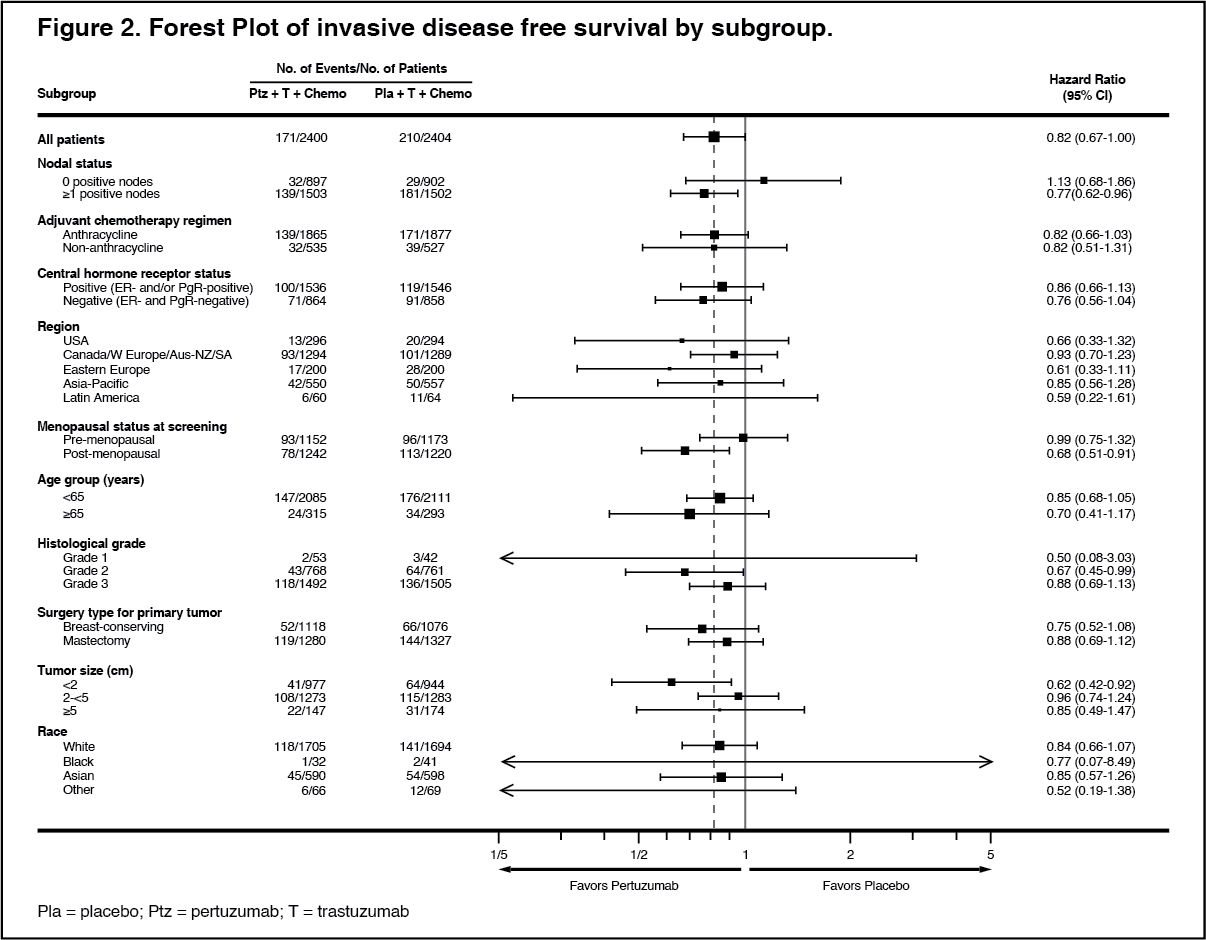 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image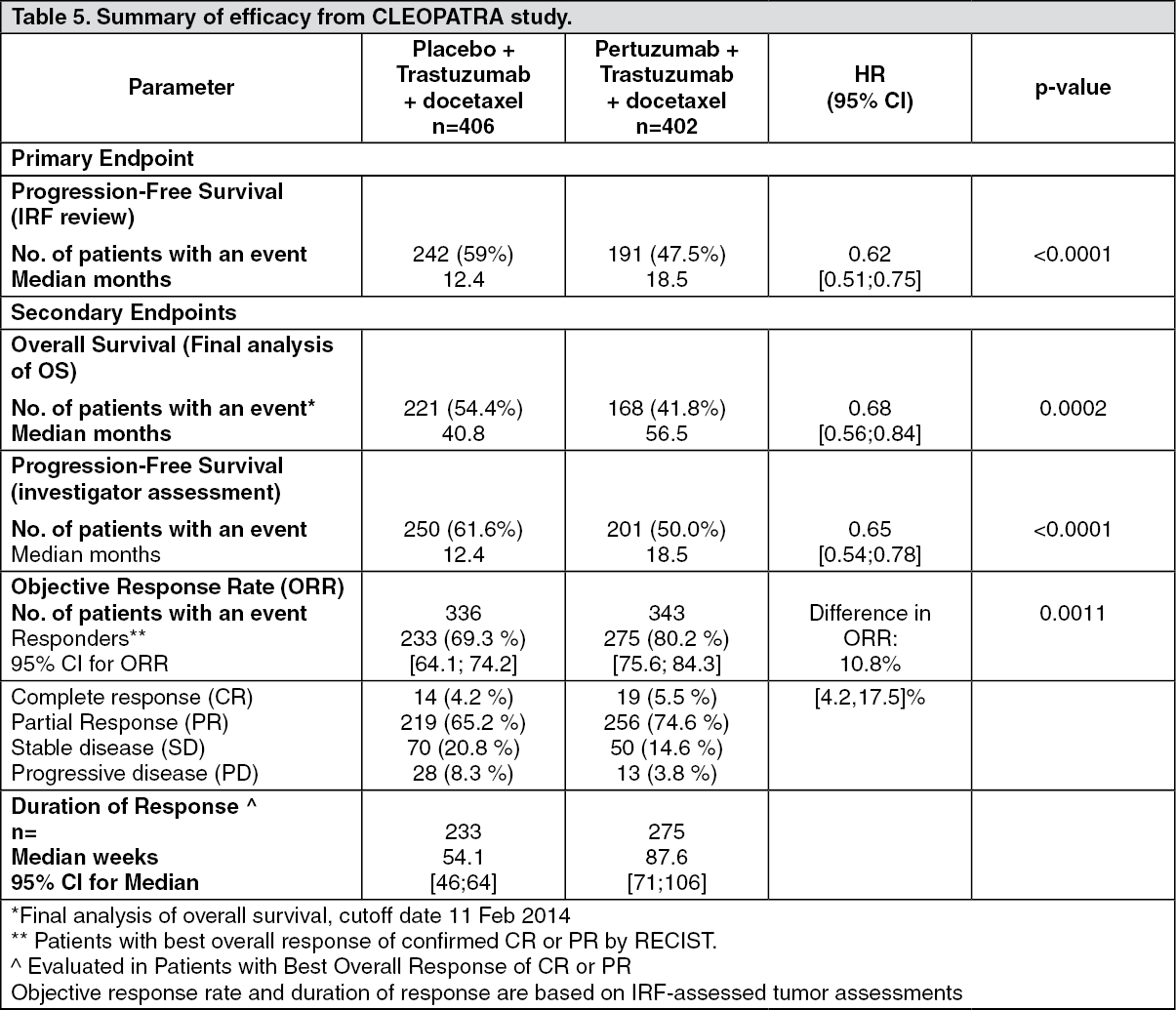 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image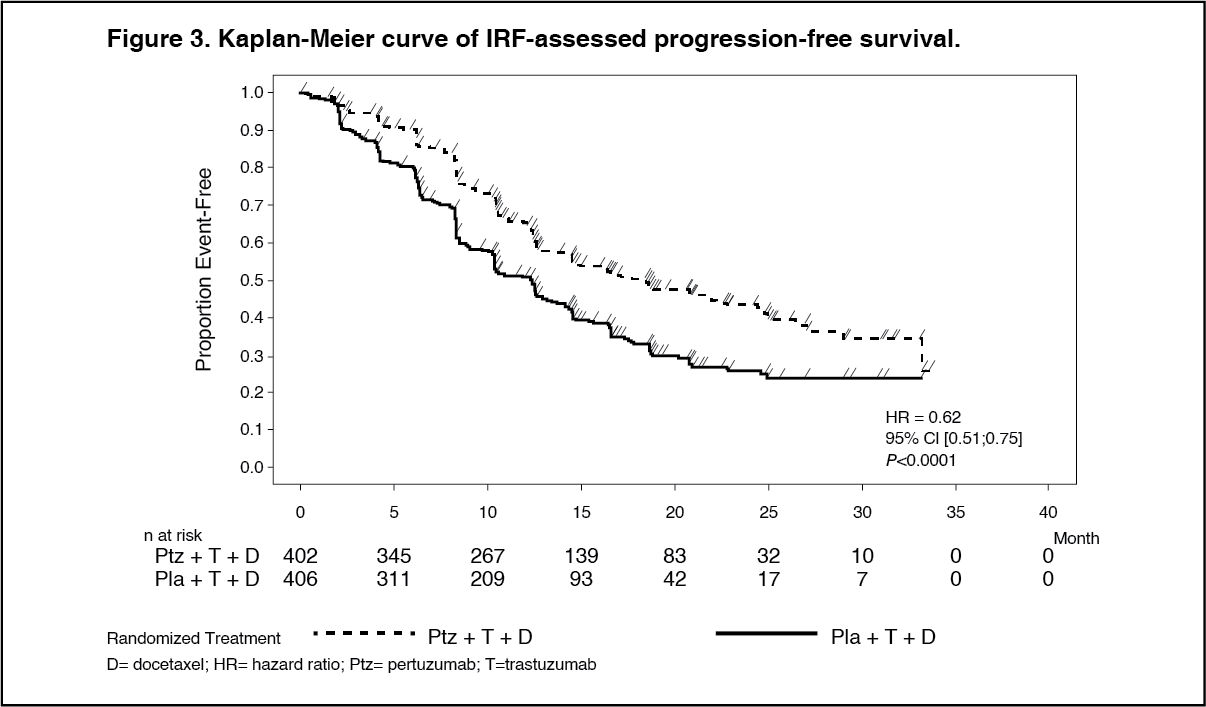 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image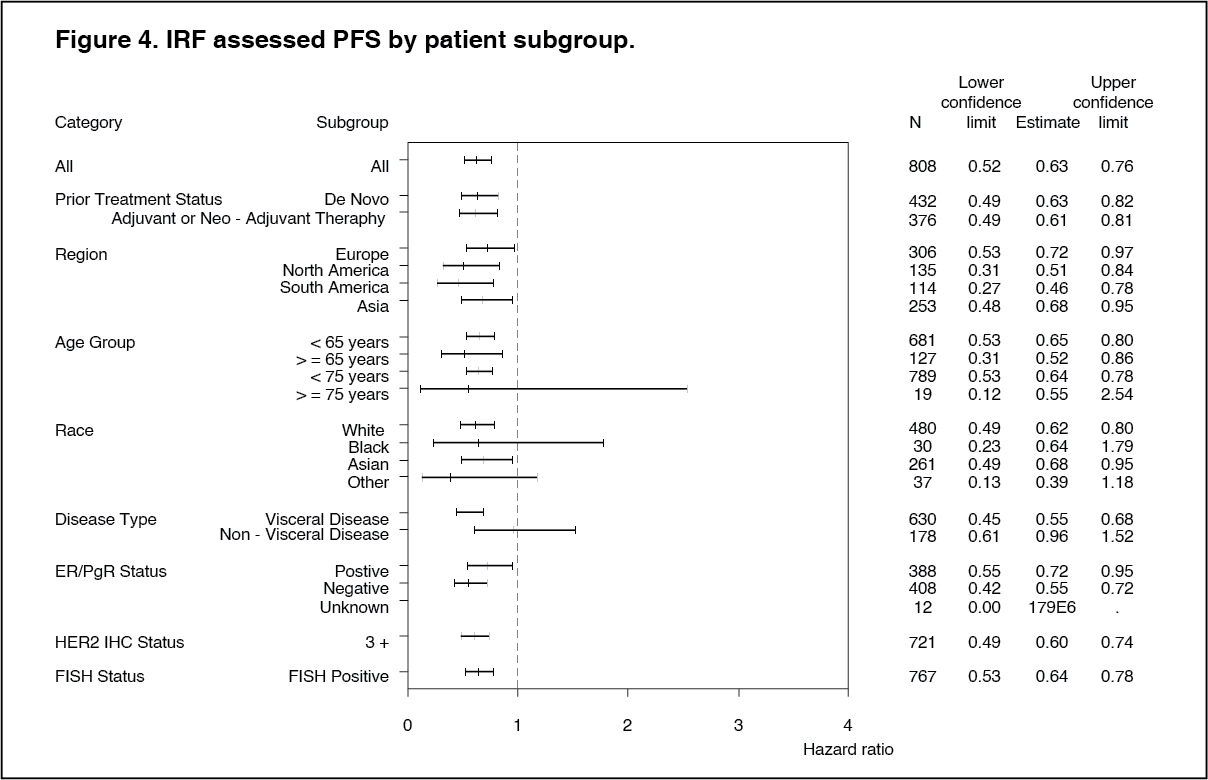 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image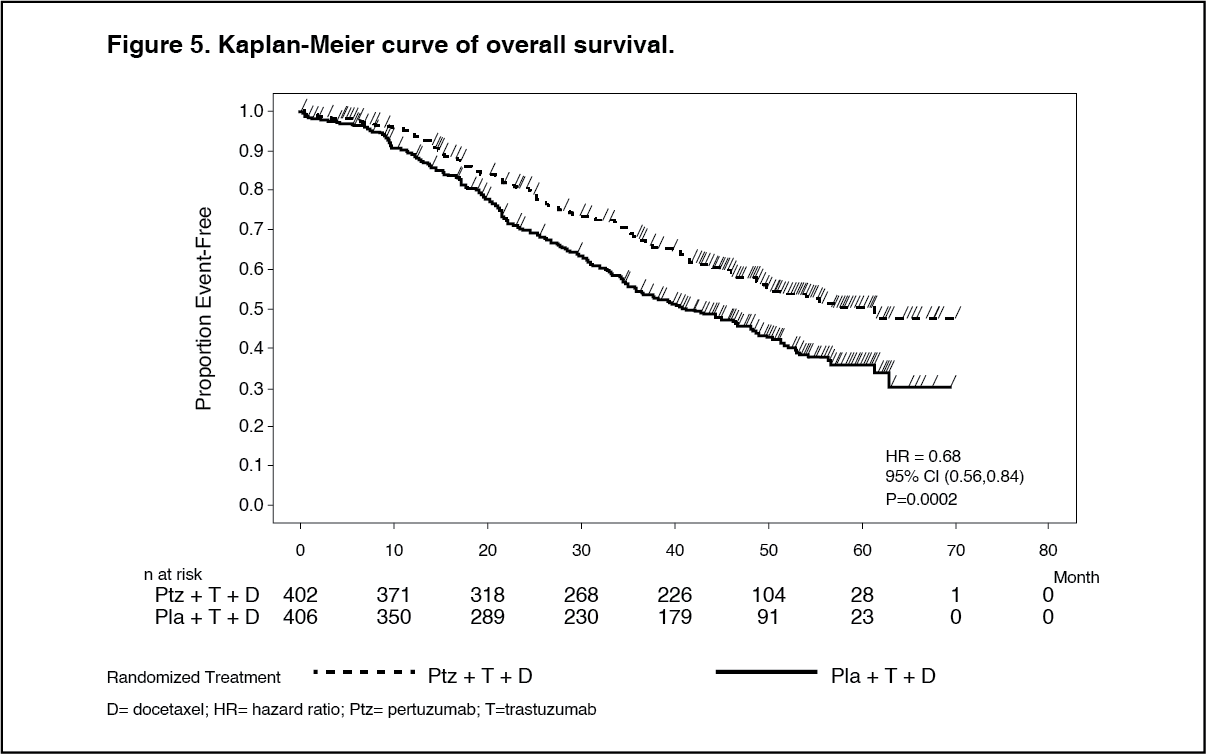 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image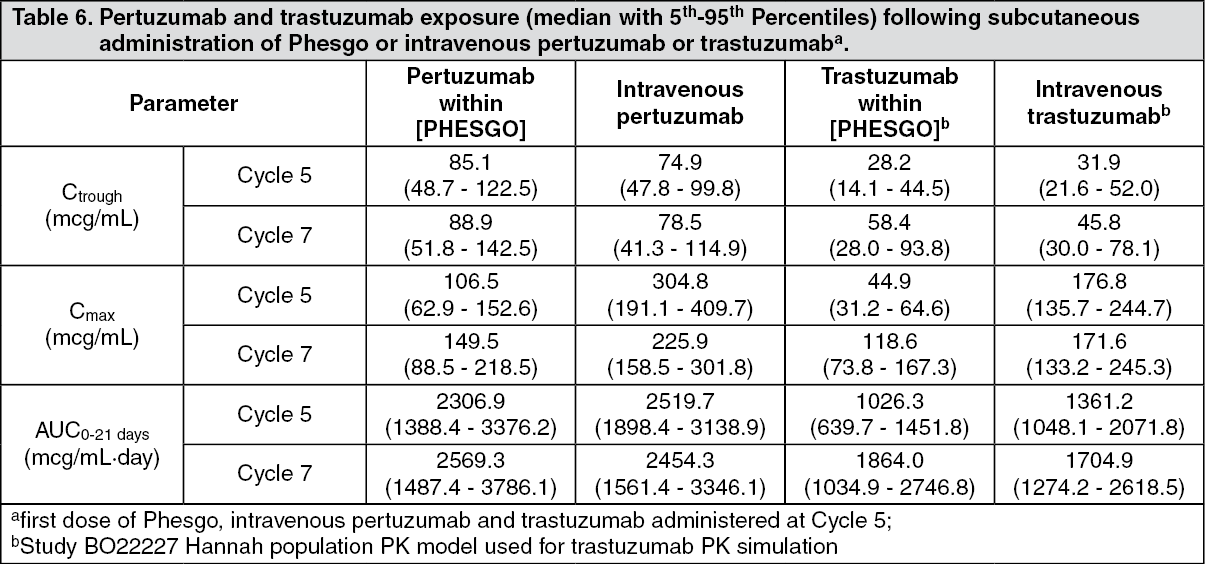 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out