


 Sign Out
Sign Out

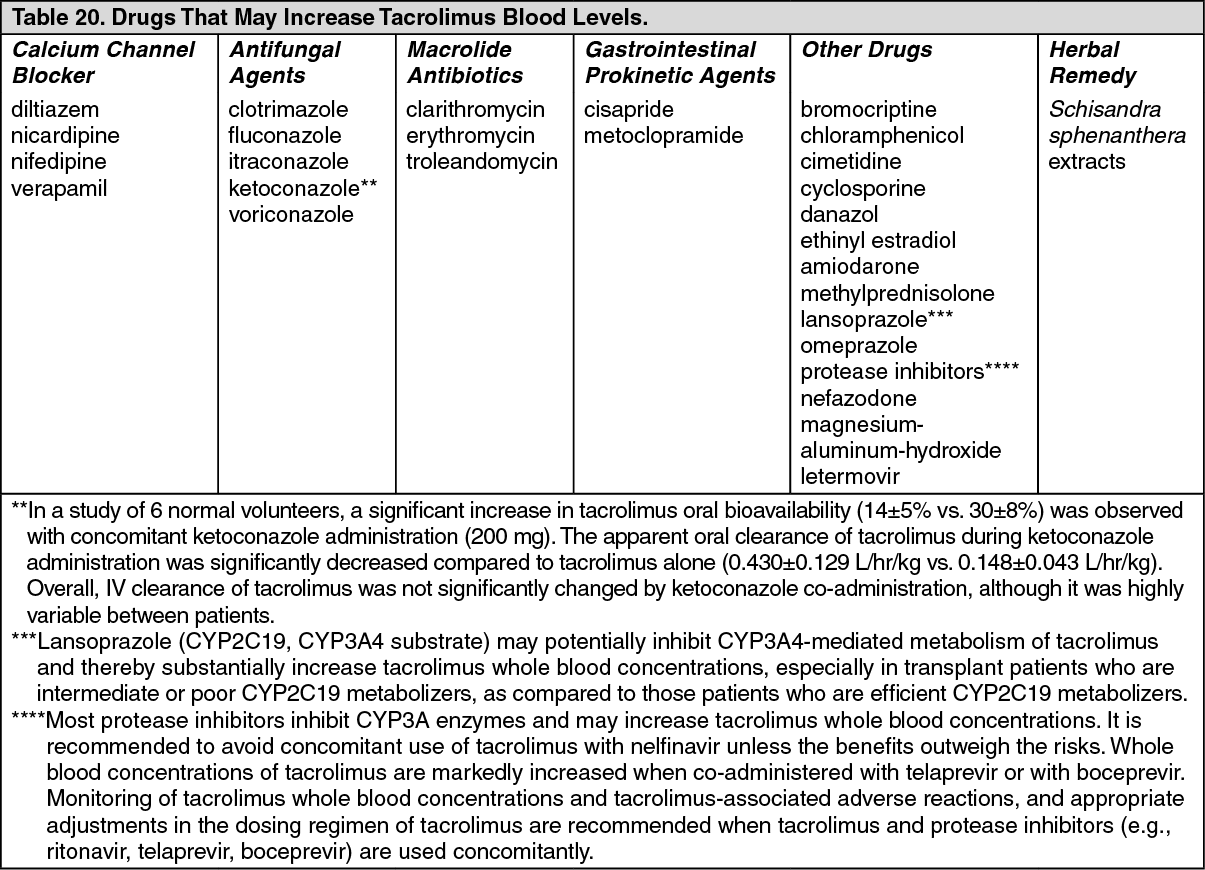
Drugs that May Alter Tacrolimus Concentrations: Since tacrolimus is metabolized mainly by the CYP3A enzyme systems, substances known to inhibit these enzymes may decrease the metabolism of tacrolimus with resultant increases in whole blood or plasma levels. Drugs known to induce these enzyme systems may result in an increased metabolism of tacrolimus and decreased whole blood or plasma levels. Monitoring of blood concentrations and appropriate dosage adjustments are essential when such drugs are used concomitantly. (See Table 20.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSignificant tacrolimus dose reductions and prolongation of dosing interval may be required in order to maintain similar tacrolimus exposure when co-administered with strong CYP3A4 inhibitors, particularly telaprevir. Rapid increase in tacrolimus level may occur when co-administered with CYP3A4 inhibitors. Cases have been reported in which a sharp rise in tacrolimus levels occurred very rapidly, as early as within 1-3 days after co-administration with a strong CYP3A4 inhibitor, clarithromycin, despite immediate reduction of tacrolimus dose. Therefore early, within the first few days of co-administration, and frequent continued monitoring of tacrolimus blood levels, as well as monitoring for renal function, for QT prolongation with ECG, and for other side effects is strongly recommended. (See Table 21.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSt. John's wort (Hypericum perforatum) induces CYP3A4 and P-glycoprotein. Since tacrolimus is a substrate for CYP3A4, there is the potential that the use of St. John's wort in patients receiving Prograf could result in reduced tacrolimus levels.
In a single-dose crossover study in healthy volunteers, co-administration of tacrolimus and magnesium-aluminum-hydroxide resulted in a 21% increase in the mean tacrolimus AUC and a 10% decrease in the mean tacrolimus Cmax relative to tacrolimus administration alone.
In a study of 6 normal volunteers, a significant decrease in tacrolimus oral bioavailability (14±6% vs. 7±3%) was observed with concomitant rifampin administration (600 mg). In addition, there was a significant increase in tacrolimus clearance (0.036±0.008 L/hr/kg vs. 0.053±0.010 L/hr/kg) with concomitant rifampin administration.
Interaction studies with drugs used in HIV therapy have not been conducted. However, care should be exercised when drugs that are nephrotoxic (e.g., ganciclovir) or that are metabolized by CYP3A (e.g., nelfinavir, ritonavir) are administered concomitantly with tacrolimus.
Based on a clinical study of 5 liver transplant recipients, co-administration of tacrolimus with nelfinavir increased blood concentrations of tacrolimus significantly and, as a result, a reduction in the tacrolimus dose by an average of 16-fold was needed to maintain mean trough tacrolimus blood concentrations of 9.7 ng/mL. Thus, frequent monitoring of tacrolimus blood concentrations and appropriate dosage adjustments are essential when nelfinavir is used concomitantly.
In a single dose study in 9 healthy volunteers, co-administration of tacrolimus (0.5 mg single dose) with telaprevir (750 mg three times daily for 13 days) increased the tacrolimus dose normalized Cmax by 9.3-fold and AUC by 70-fold compared to tacrolimus alone.
In a single dose study in 12 subjects, co-administration of tacrolimus (0.5 mg single dose) with boceprevir (800 mg three times daily for 11 days) increased tacrolimus Cmax by 9.9-fold and AUC by 17-fold compared to tacrolimus alone.
Tacrolimus may affect the pharmacokinetics of other drugs (e.g., phenytoin) and increase their concentration. Grapefruit juice affects CYP3A-mediated metabolism and should be avoided (see DOSAGE & ADMINISTRATION).
Following co-administration of tacrolimus and sirolimus (2 or 5 mg/day) in stable renal transplant patients, mean tacrolimus AUC0-12 and Cmin decreased approximately by 30% relative to tacrolimus alone. Mean tacrolimus AUC0-12 and Cmin following co-administration of 1 mg/day of sirolimus decreased approximately 3% and 11%, respectively. The safety and efficacy of tacrolimus used in combination with sirolimus for the prevention of graft rejection has not been established and is not recommended.
Other Drug Interactions: Immunosuppressants may affect vaccination. Therefore, during treatment with Prograf, vaccination may be less effective. The use of live vaccines should be avoided; live vaccines may include, but are not limited to measles, mumps, rubella, oral polio, BCG, yellow fever, and TY 21a typhoid.
At a given MMF dose, mycophenolic acid (MPA) exposure is higher with Prograf co-administration than with cyclosporine co-administration due to the differences in the interruption of the enterohepatic recirculation of MPA. Clinicians should be aware that there is also a potential for increased MPA exposure after crossover from cyclosporine to tacrolimus in patients concomitantly receiving MMF or MPA.
Impact of direct-acting antiviral (DAA) therapy. The pharmacokinetics of tacrolimus may be impacted by changes in liver function during DAA therapy, related to clearance of HCV virus. A close monitoring and potential dose adjustment of tacrolimus is warranted to ensure continued efficacy and safety.