


 Sign Out
Sign Out

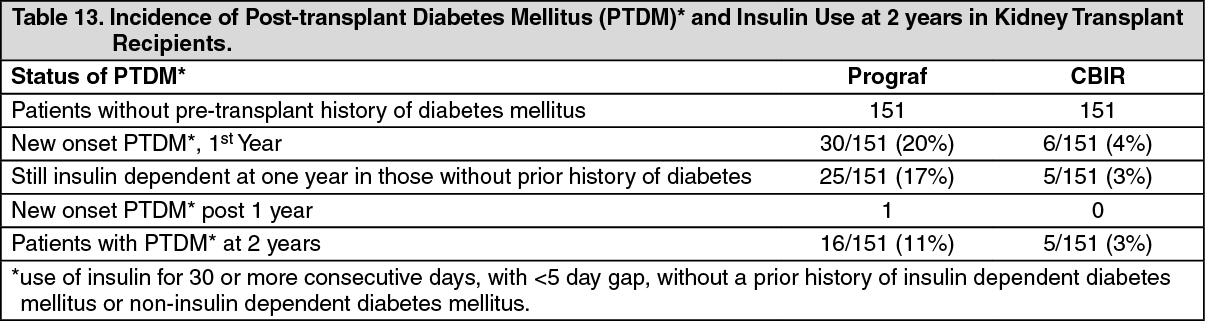
Post-Transplant Diabetes Mellitus: Insulin-dependent post-transplant diabetes mellitus (PTDM) was reported in 20% of Prograf-treated kidney transplant patients without pre-transplant history of diabetes mellitus in the Phase III study (see Tables 13 and 14 as follows). The median time to onset of PTDM was 68 days. Insulin dependence was reversible in 15% of these patients at one year and in 50% at two years post-transplant. Black and Hispanic kidney transplant patients were at an increased risk of development of PTDM. (See Tables 13 and 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image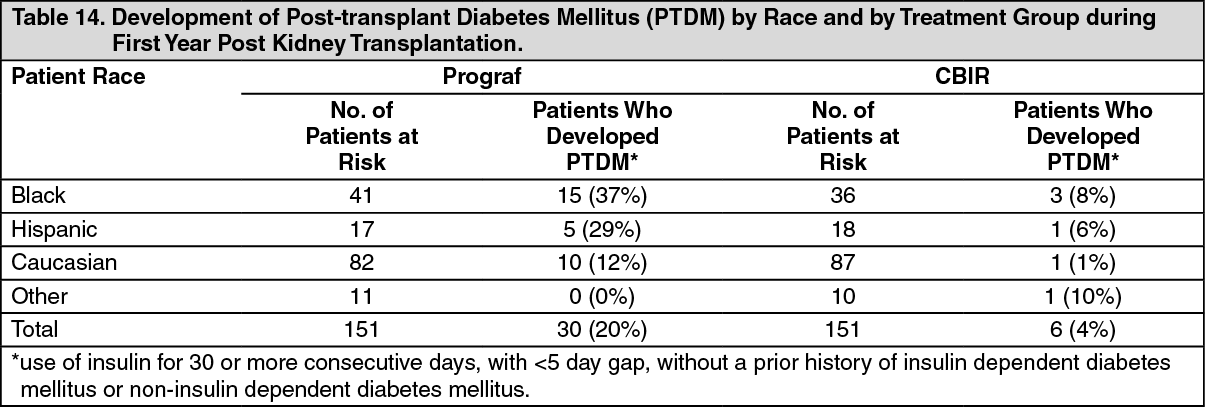 Click on icon to see table/diagram/image
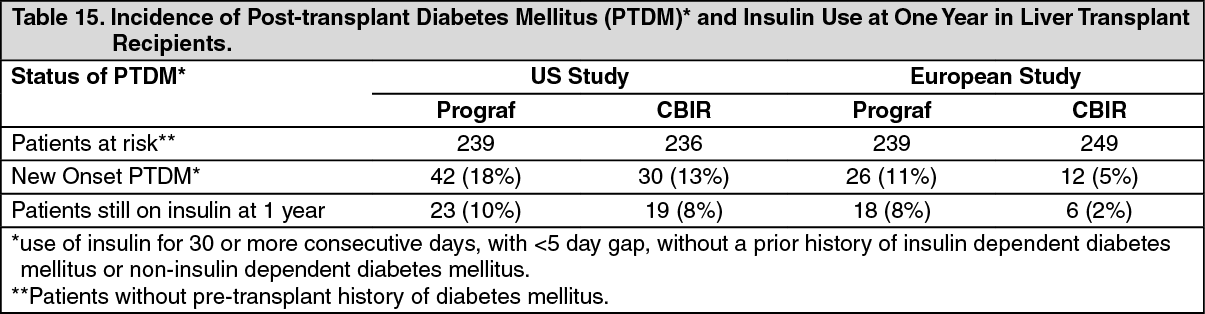
Click on icon to see table/diagram/imageInsulin-dependent post-transplant diabetes mellitus was reported in 18% and 11% of Prograf-treated liver transplant patients and was reversible in 45% and 31% of these patients at one year post transplant, in the U.S. and European randomized studies, respectively (see Table 15 as follows). Hyperglycemia was associated with the use of Prograf in 47% and 33% of liver transplant recipients in the U.S. and European randomized studies, respectively, and may require treatment (see ADVERSE REACTIONS). (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNephrotoxicity: Prograf can result in both acute and chronic renal function impairment in transplant patients due to its vasoconstrictive effect on renal vasculature, toxic tubulopathy and tubularinterstitial effects. Prograf can cause nephrotoxicity, particularly when used in high doses. Nephrotoxicity was reported in approximately 52% of kidney transplantation patients and in 40% and 36% of liver transplantation patients receiving Prograf in the U.S. and European randomized trials, respectively (see ADVERSE REACTIONS).
Acute renal impairment can result in high serum creatinine, hyperkalemia, decreased secretion of urea, hyperuricemia, and is usually reversible. Chronic renal impairment is characterized by progressive renal dysfunction, increased blood urea and proteinuria. Patients with impaired renal function should be monitored closely as the dosage of Prograf may need to be transiently reduced or discontinued. In patients with persistent elevations of serum creatinine who are unresponsive to dosage adjustments, consideration should be given to changing to another immunosuppressive therapy. Acute renal impairment without active intervention may progress to chronic renal impairment.
Concurrent use of Prograf with other known nephrotoxic drugs could result in potentiation of nephrotoxicity. When concurrent use of tacrolimus with other known nephrotoxic drugs is required, monitor renal function and tacrolimus blood concentrations frequently, and dose adjustments of both tacrolimus and/or concomitant medications should be considered upon initiation, throughout concurrent treatment and at discontinuation of such concomitant drugs. In particular, to avoid excess nephrotoxicity, Prograf should not be used simultaneously with cyclosporine. Prograf or cyclosporine should be discontinued at least 24 hours prior to initiating the other. In the presence of elevated Prograf or cyclosporine concentrations, dosing with the other drug usually should be further delayed (see INTERACTIONS).
Hyperkalemia: Mild to severe hyperkalemia was reported in 31% of kidney transplant recipients and in 45% and 13% of liver transplant recipients treated with Prograf in the U.S. and European randomized trials, respectively, and may require treatment (see ADVERSE REACTIONS). Serum potassium levels should be monitored and potassium-sparing diuretics should not be used during Prograf therapy (see PRECAUTIONS).
Live vaccine: As with other immunosuppressants, response to vaccination during treatment with tacrolimus may be less effective. The use of live attenuated vaccines should be avoided.
Neurotoxicity: Prograf can cause neurotoxicity, particularly when used in high doses.
Neurotoxicity, including tremor, headache, and other changes in motor function, mental status, and sensory function were reported in approximately 55% of liver transplant recipients in the two randomized studies. Tremor occurred more often in Prograf-treated kidney transplant patients (54%) compared to cyclosporine-treated patients. The incidence of other neurological events in kidney transplant patients was similar in the two treatment groups (see ADVERSE REACTIONS). Tremor and headache have been associated with high whole-blood concentrations of tacrolimus and may respond to dosage adjustment. Seizures have occurred in adult and pediatric patients receiving Prograf (see ADVERSE REACTIONS). Coma and delirium also have been associated with high plasma concentrations of tacrolimus. Patients treated with tacrolimus have been reported to develop posterior reversible encephalopathy syndrome (PRES). Symptoms indicating PRES include headache, altered mental status, seizures, visual disturbances and hypertension. Diagnosis may be confirmed by radiological procedure. If PRES is suspected or diagnosed, blood pressure control should be maintained and immediate reduction of immunosuppression is advised. This syndrome is characterized by reversal of symptoms upon reduction or discontinuation of immunosuppression.
Malignancy and Lymphoproliferative Disorders: As in patients receiving other immunosuppressants, patients receiving Prograf are at increased risk of developing lymphomas and other malignancies, particularly of the skin. The risk appears to be related to the intensity and duration of immunosuppression rather than to the use of any specific agent. A Lymphoproliferative disorder (LPD) related to Epstein-Barr Virus (EBV) infection has been reported in immunosuppressed organ transplant recipients. The risk of LPD appears greatest in young children who are at risk for primary EBV infection while immunosuppressed or who are switched to Prograf following long-term immunosuppression therapy.
Because of the danger of over-suppression of the immune system which can increase susceptibility to infection, combination immunosuppressant therapy should be used with caution.
Latent Viral Infections: Immunosuppressed patients are at increased risk for opportunistic infections, including latent viral infections. These include BK virus associated nephropathy, JC virus associated progressive multifocal leukoencephalopathy, and CMV infection that have been observed in patients receiving tacrolimus. These infections may lead to serious, including fatal, outcomes.
Anaphylactic Reactions: A few patients receiving Prograf injection have experienced anaphylactic reactions. Although the exact cause of these reactions is not known, other drugs with castor oil derivatives in the formulation have been associated with anaphylaxis in a small percentage of patients. Because of this potential risk of anaphylaxis, Prograf injection should be reserved for patients who are unable to take Prograf capsules.
Patients receiving Prograf injection should be under continuous observation for at least the first 30 minutes following the start of the infusion and at frequent intervals thereafter. If signs or symptoms of anaphylaxis occur, the infusion should be stopped. An aqueous solution of epinephrine should be available at the bedside as well as a source of oxygen.
Pure Red Cell Aplasia: Cases of pure red cell aplasia (PRCA) have been reported in patients treated with tacrolimus. A mechanism for tacrolimus-induced PRCA has not been elucidated. All patients reported risk factors for PRCA such as parvovirus B19 infection, underlying disease, or concomitant medications associated with PRCA. If PRCA is diagnosed, discontinuation of Prograf should be considered.
Use with CYP3A4 Inhibitors and Inducers Including Those That Prolong QT: Co-administration with strong CYP3A4-inhibitors (e.g., telaprevir, boceprevir, ritonavir, ketoconazole, itraconazole, voriconazole, clarithromycin) and strong inducers (e.g., rifampin, rifabutin) is not recommended without adjustments in the dosing regimen of tacrolimus and subsequent close monitoring of tacrolimus whole blood trough concentrations and tacrolimus-associated adverse reactions.
Early and frequent continued monitoring of tacrolimus blood levels within the first few days of co-administration, as well as monitoring for renal function, for QT prolongation with ECG, and for other side effects is strongly recommended when co-administered with CYP3A4 inhibitors (see INTERACTIONS). Use of tacrolimus with amiodarone has been reported to result in increased tacrolimus whole blood concentrations with or without concurrent QT prolongation.
Use with herbal preparation: Herbal preparations containing St. John's wort (Hypericum perforatum) should be avoided when taking tacrolimus due to the risk of interactions that lead to decrease in blood concentrations of tacrolimus and reduced clinical effect of tacrolimus (see INTERACTIONS).