


 Sign Out
Sign Out
Data to determine the frequency of ceftriaxone ADRs was derived from clinical trials.
Tabulated summary of adverse drug reactions from clinical trials: Adverse drug reactions from clinical trials (Table 2) are listed by MedDRA system organ class. The corresponding frequency category for each adverse drug reaction is based on the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1000). (See Table 2.)
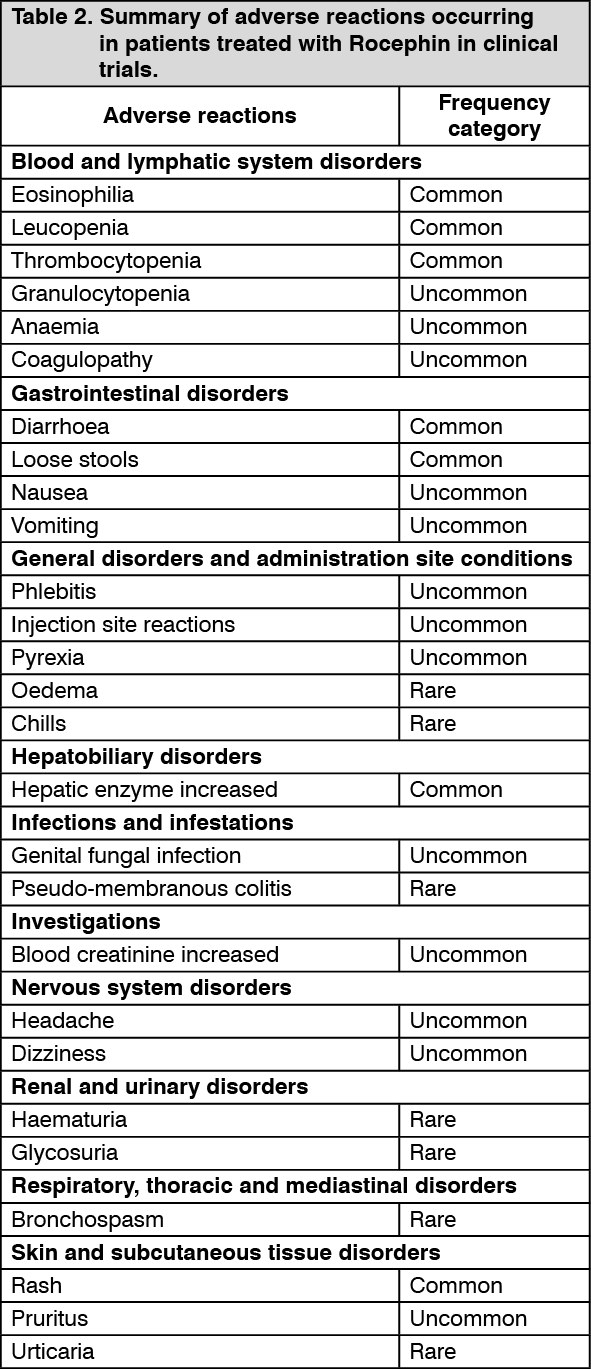 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePost Marketing Experience: The following adverse drug reactions have been identified from post-marketing experience with Rocephin. These reactions are reported from a population of uncertain size, therefore, it is not always possible to reliably estimate their frequency and/or establish a causal relationship to drug exposure.
Systemic side effects: Gastrointestinal complaints pancreatitis, stomatitis and glossitis.
Hematological changes isolated cases of agranulocytosis (< 500/mm3) have been reported, most of them after 10 days of treatment and following total doses of 20 g or more.
Skin reactions acute generalized exanthematous pustulosis (AGEP), isolated cases of severe cutaneous adverse reactions (erythema multiforme, Stevens-Johnson syndrome or Lyell's Syndrome/toxic epidermal necrolysis) have been reported.
Nervous system disorders: convulsion, encephalopathy.
Reversible encephalopathy has been reported with the use of cephalosporins, including ceftriaxone, particularly when high doses are administered in patients with renal impairment and additional predisposing factors such as older age, pre-existing central nervous system disorders.
Infections and Infestations: superinfection.
Other, rare side effects: symptomatic precipitation of ceftriaxone calcium salt in the gallbladder, kernicterus, oliguria and anaphylactic or anaphylactoid reactions.
Interaction with calcium: Two in vitro studies, one using adult plasma and the other neonatal plasma from umbilical cord blood have been carried out to assess interaction of ceftriaxone and calcium. Ceftriaxone concentrations up to 1 mM (in excess of concentrations achieved in vivo following administration of 2 grams ceftriaxone infused over 30 minutes) were used in combination with calcium concentrations up to 12 mM (48 mg/dL). Recovery of ceftriaxone from plasma was reduced with calcium concentrations of 6 mM (24 mg/dL) or higher in adult plasma or 4 mM (16 mg/dL) or higher in neonatal plasma. This may be reflective of ceftriaxone-calcium precipitation.
A small number of cases of fatal outcomes in which a crystalline material was observed in the lungs and kidneys at autopsy have been reported in neonates receiving Rocephin and calcium containing fluids. In some of these cases, the same intravenous infusion line was used for both Rocephin and calcium-containing fluids and in some a precipitate was observed in the intravenous infusion line. At least one fatality has been reported in a neonate in whom Rocephin and calcium-containing fluids were administered at different time points via different intravenous lines; no crystalline material was observed at autopsy in this neonate. There have been no similar reports in patients other than neonates (see General under Precautions).
Cases of ceftriaxone precipitation in the urinary tract have been reported, mostly in children treated with high doses (e.g. ≥ 80 mg/kg/day or total doses exceeding 10 grams) and who have other risk factors (e.g. dehydration, confinement to bed). This event may be asymptomatic or symptomatic, and may lead to ureteric obstruction and postrenal acute renal failure but is usually reversible upon discontinuation of Rocephin.
Local side effects: In rare cases, phlebitis reactions occurred after i.v. administration. These may be minimized by slow (2-4 minutes) injection.
Investigations: Coombs test false positive, galactosemia test false positive, non-enzymatic methods for glucose determination false positive.
View ADR Monitoring Form