Pharmacotherapeutic group: Antibacterials for systemic use, Third-generation cephalosporins.
ATC code: J01DD04.
PHARMACOLOGY: Pharmacodynamics: Mechanism of Action: The bactericidal activity of ceftriaxone results from inhibition of bacterial cell wall synthesis. Ceftriaxone exerts in-vitro activity against a wide range of gram-negative and gram-positive micro-organisms. Ceftriaxone is highly stable to most β-lactamases, both penicillinases and cephalosporinases, of gram-positive and gram-negative bacteria. Ceftriaxone is usually active against the following micro-organisms in vitro and in clinical infections (see Indications/Uses): Gram-positive aerobes:
Staphylococcus aureus (methicillin-sensitive), Staphylococci coagulase-negative,
Streptococcus pyogenes (β-hemolytic, group A),
Streptococcus agalactiae (β-hemolytic, group B), β-hemolytic Streptococci (non-group A or B),
Streptococcus viridans,
Streptococcus pneumoniae.
Note: Methicillin-resistant
Staphylococcus spp. is resistant to cephalosporins, including ceftriaxone. In general,
Enterococcus faecalis,
Enterococcus faecium and
Listeria monocytogenes are resistant.
Gram-negative aerobes:
Acinetobacter lwoffi,
Acinetobacter anitratus (mostly
A. baumanii)*,
Aeromonas hydrophila,
Alcaligenes faecalis,
Alcaligenes odorans, Alcaligenes-like bacteria,
Borrelia burgdorferi,
Capnocytophaga spp.,
Citrobacter diversus (including
C. amalonaticus),
Citrobacter freundii*,
Escherichia coli,
Enterobacter aerogenes*,
Enterobacter cloacae*,
Enterobacter spp. (other)*,
Haemophilus ducreyi,
Haemophilus influenzae,
Haemophilus parainfluenzae,
Hafnia alvei,
Klebsiella oxytoca,
Klebsiella pneumoniae**,
Moraxella catarrhalis (former
Branhamella catarrhalis),
Moraxella osloensis,
Moraxella spp. (other),
Morganella morganii,
Neisseria gonorrhoea,
Neisseria meningitidis,
Pasteurella multocida,
Plesiomonas shigelloides,
Proteus mirabilis,
Proteus penneri*,
Proteus vulgaris*,
Pseudomonas fluorescens*,
Pseudomonas spp. (other)*,
Providentia rettgeri*,
Providentia spp. (other),
Salmonella typhi,
Salmonella spp. (non-typhoid),
Serratia marcescens*,
Serratia spp. (Other)*,
Shigella spp.,
Vibrio spp.,
Yersinia enterocolitica,
Yersinia spp. (other).
* Some isolates of these species are resistant to ceftriaxone, mainly due to the production of the chromosomally encoded β-lactamase.
** Some isolates of these species are resistant due to production of extended spectrum, plasmid-mediated β-lactamase.
Note: Many strains of the previously mentioned micro-organisms that are multiple resistant to other antibiotics, e.g. amino-penicillins and ureido-penicillins, older cephalosporins and aminoglycosides, are susceptible to ceftriaxone.
Treponema pallidum is sensitive in vitro and in animal experiments. Clinical investigations indicate that primary and secondary syphilis respond well to ceftriaxone therapy. With a few exceptions clinical
P. aeruginosa isolates are resistant to ceftriaxone.
Anaerobic organisms:
Bacteroides spp. (bile-sensitive)*,
Clostridium spp. (excluding
C. difficile),
Fusobacterium nucleatum,
Fusobacterium spp. (other),
Gaffkia anaerobica (formerly Peptococcus),
Peptostreptococcus spp.
* Some isolates of these species are resistant to ceftriaxone due to β-lactamase-production.
Note: Many strains of β-lactamase-producing
Bacteroides spp. (notably
B. fragilis) are resistant.
Clostridium difficile is resistant.
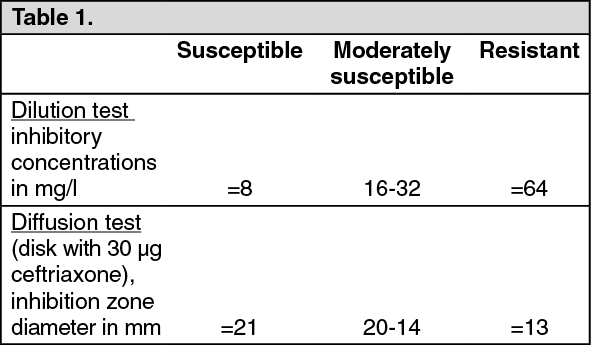
Susceptibility to ceftriaxone can be determined by the disk diffusion test or by the agar or broth dilution test using standardised techniques for susceptibility testing such as those recommended by the National Committee for Clinical Laboratory Standards (NCCLS). The NCCLS issued the following interpretative breakpoints for ceftriaxone: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Micro-organisms should be tested with the ceftriaxone disk since it has been shown by in-vitro tests to be active against certain strains resistant to cephalosporin class disks.
Where NCCLS recommendations are not in daily use, alternative, well standardised, susceptibility-interpretative guidelines such as those issued by DIN, ICS and others may be substituted.
Pharmacokinetics: The pharmacokinetics of ceftriaxone are non-linear and all basic pharmacokinetic parameters, except the elimination half-life, are dose dependent if based on total drug concentrations, increasing less than proportionally with dose. Non-linearity is due to saturation of plasma protein binding and is therefore observed for total plasma ceftriaxone but not for free (unbound) ceftriaxone.
Absorption: Rocephin is administered as an intramuscular injection or as an IV injection or infusion.
The maximum plasma concentration after a single i.m. dose of 1 g is about 81 mg/l and is reached in 2-3 hours after administration. The area under the plasma concentration-time curve after i.m. administration is equivalent to that after i.v. administration of an equivalent dose, indicating 100% bioavailability of intramuscularly administered ceftriaxone.
After intravenous bolus administration of ceftriaxone 500 mg and 1 g, mean peak plasma ceftriaxone levels are approximately 120 and 200 mg/l respectively. After intravenous infusion of ceftriaxone 500 mg, 1 g and 2 g, the plasma ceftriaxone levels are approximately 80, 150 and 250 mg/l respectively. Following intramuscular injection, mean peak plasma ceftriaxone levels are approximately half those observed after intravenous administration of an equivalent dose.
Distribution: The volume of distribution of ceftriaxone is 7-12 l. Ceftriaxone has shown excellent tissue and body fluid penetration after a dose of 1-2 g; concentrations well above the minimal inhibitory concentrations of most pathogens responsible for infection are detectable for more than 24 hours in over 60 tissues or body fluids including lung, heart, biliary tract/liver, tonsil, middle ear and nasal mucosa, bone as well as cerebrospinal, pleural, prostatic and synovial fluids.
On intravenous administration, ceftriaxone diffuses rapidly into the interstitial fluid, where bactericidal concentrations against susceptible organisms are maintained for 24 hours (see figure).
Click on icon to see table/diagram/image
Protein binding: Ceftriaxone is reversibly bound to albumin. Plasma protein binding is about 95% at plasma concentrations below 100 mg/l. Binding is saturable and the bound portion decreases with rising concentration (up to 85% at a plasma concentration of 300 mg/l).
Penetration into particular tissues: Ceftriaxone penetrates the meninges. Penetration is greatest when the meninges are inflamed. Mean peak ceftriaxone concentrations in CSF in patients with bacterial meningitis are reported to be up to 25% of plasma levels compared to 2% of plasma levels in patients with uninflamed meninges. Peak ceftriaxone concentrations in CSF are reached approximately 4-6 hours after intravenous injection.
Ceftriaxone crosses the placental barrier and is excreted in the breast milk at low concentrations.
Metabolism: Ceftriaxone is not metabolised systemically; but is converted to inactive metabolites by the gut flora.
Elimination: Total plasma clearance is 10-22 ml/min. Renal clearance is 5-12 ml/min.
50-60% of ceftriaxone is excreted unchanged in the urine, while 40-50% is excreted unchanged in the bile. The elimination half-life in adults is about 8 hours.
Pharmacokinetics in Special Populations: Pediatric Population: The half-life of ceftriaxone is prolonged in neonates. From birth to 14 days of age, the levels of free ceftriaxone may be further increased by factors such as reduced glomerular filtration and altered protein binding. During childhood, the half-life is lower than in neonates or adults.
The plasma clearance and volume of distribution of total ceftriaxone are greater in neonates, infants and children than in adults.
Geriatric Population: In elderly persons aged over 75 years the average elimination half-life is usually two to three times that of young adults.
Renal Impairment: In patients with renal impairment, the pharmacokinetics of ceftriaxone are only minimally altered and the elimination half-life is only slightly increased, (less than two fold), even in patients with severely impaired renal function. The modest increase in half-life in renal impairment is explained by a compensatory increase in non-renal clearance, resulting from a decrease in protein binding and corresponding increase in non-renal clearance of total ceftriaxone.
Hepatic Impairment: In patients with hepatic dysfunction, the pharmacokinetics of ceftriaxone are only minimally altered and the elimination half-life is only slightly increased, (less than two fold).
In this patients-population, the elimination half-life of ceftriaxone is not increased, due to a compensatory increase in renal clearance. This is also due to an increase in plasma free fraction of ceftriaxone contributing to the observed paradoxical increase in total drug clearance, with an increase in volume of distribution paralleling that of total clearance.
Toxicology: NONCLINICAL Safety: Non clinical data reveal no special hazards for humans based on conventional studies of safety pharmacology, acute and repeated dose toxicity, genotoxicity, or toxicity to reproduction.
Carcinogenicity: No carcinogenicity studies have been performed to establish the carcinogenic potential of Rocephin.
Genotoxicity: No evidence of mutagenicity has been found in vitro or in vivo.
Impairment of Fertility: No effect on male or female fertility has been detected.
Reproductive toxicity: Reproductive studies in animals have shown no evidence of embryotoxicity, fetotoxicity, teratogenicity, birth or perinatal and postnatal development. In primates, no embryotoxicity or teratogenicity has been observed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image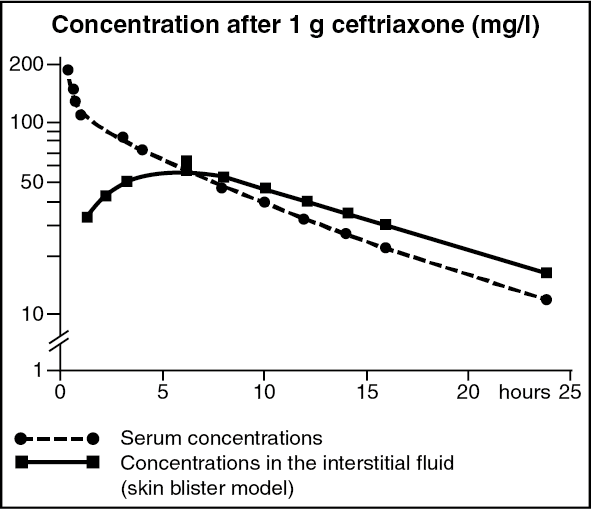 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out