


 Sign Out
Sign Out

In adult patients with newly diagnosed Ph+ CML-CP: The data reported as follows reflect exposure to Tasigna from a randomized Phase III study in adult patients with newly diagnosed Ph+ CML in chronic phase treated at the recommended dose of 300 mg twice daily (n=279). The median time on treatment was 60.5 months (range 0.1 to 70.8 months).
Non-hematologic adverse drug reactions (ADRs) reported with very common frequency (≥10%) were rash, pruritus, headache, nausea, fatigue, alopecia, myalgia, and upper abdominal pain. Most of these ADRs were mild to moderate in severity (Grade 1 or 2). Constipation, diarrhoea, dry skin, muscle spasms, arthralgia, abdominal pain, peripheral oedema, vomiting and asthenia were observed less commonly (<10% and ≥5%) and have been of mild to moderate severity, manageable and generally did not require dose reduction. Pleural and pericardial effusions, regardless of causality, occurred in 2% and <1% of patients, respectively, receiving Tasigna 300 mg twice daily. Gastrointestinal haemorrhage, regardless of causality, was reported in 3% of these patients.
The change from baseline in mean time-averaged QTcF interval at steady-state in the nilotinib recommended dose of 300 mg twice daily was 6 msec. In the nilotinib 400 mg twice daily group and the imatinib 400 mg once daily group the change from baseline in mean time-averaged QTcF interval at steady-state was 6 msec and 3 msec, respectively. No patient had an absolute QTcF of >500 msec while on study drug in any of the Tasigna treatment groups and no events of Torsades de Pointes were observed. QTcF increase from baseline that exceeds 60 msec was observed in 5 patients while on Tasigna (one in the 300 mg twice daily treatment group and four in the 400 mg twice daily treatment group).
No patients in any treatment group had a left ventricular ejection fraction (LVEF) <45% during treatment. Also, there were no patients with 15% or greater decrease from baseline in LVEF.
No sudden deaths have been reported in any treatment group.
In the nilotinib 300 mg twice daily group, haematologic ADRs include myelosuppression: thrombocytopenia (18%), neutropenia (15%), and anaemia (8%). Biochemistry ADRs include alanine aminotransferase increased (24%), hyperbilirubinaemia (16%), aspartate aminotransferase increased (12%), lipase increased (11%), blood bilirubin increased (10%), hyperglycaemia (4%), hypercholesterolaemia (3%), and hypertriglyceridaemia (<1%). See Table 12 for Grade 3/4 laboratory abnormalities.
Discontinuation due to adverse drug reactions was observed in 10% of patients.
In adult patients with resistant or intolerant Ph+ CML-CP and CML-AP: The data reported as follows reflect exposure to Tasigna in 458 adult patients with Ph+ CML-CP (n=321) and CML-AP (n=137) resistant to or intolerant to at least one prior therapy including imatinib in an open-label multicenter study treated at the recommended dose of 400 mg twice daily.
Non-haematologic ADRs reported with very common frequency (≥10% in the combined CML-CP and CML-AP patient populations) were rash, pruritus, nausea, fatigue, headache, constipation, diarrhoea, vomiting and myalgia. Most of these ADRs were mild to moderate in severity. Alopecia, muscle spasms, decreased appetite, arthralgia, bone pain, abdominal pain, peripheral oedema and asthenia were observed less frequently (<10% and >5%) and have been of mild to moderate severity (Grade 1 or 2).
Pleural and pericardial effusions as well as complications of fluid retention occurred in <1% of patients receiving Tasigna. Cardiac failure was observed in <1% of patients. Gastrointestinal and central nervous system (CNS) haemorrhage was reported in 1% and <1% of patients, respectively.
QTcF exceeding 500 msec was observed in this study in 4 patients (<1%). No episodes of Torsades de Pointes (transient or sustained) were observed.
Haematologic ADRs include myelosuppression: thrombocytopenia (31%), neutropenia (17%), and anaemia (14%). See Table 12 for Grade 3/4 laboratory abnormalities.
Discontinuation due to adverse drug reactions was observed in 16% of CP and 10% of AP patients.
In adult patients with Ph+ CML-CP who have not achieved a molecular response greater than or equal to a 4.5-log reduction with imatinib treatment: The data reported as follows were generated in a randomized, open-label, Phase III study where adult male and female patients diagnosed with Ph+ CML-CP and after two years of imatinib therapy were exposed to Tasigna 400 mg twice daily versus imatinib 400 mg or 600 mg once daily for 48 months. Patients randomized to the imatinib arm received the same dose of imatinib as prior to randomization. The median duration of exposure was 47.2 months in the Tasigna arm and 37.0 months and 26.7 months in the 400 mg and 600 mg dose cohorts of the imatinib arm, respectively.
The adverse drug reactions reported by at least 20% of the patients in the Tasigna group and more frequently compared to the imatinib group were headache, rash, and pruritus. A greater proportion of patients in the Tasigna group reported adverse events (AEs) leading to discontinuation and AEs requiring dose adjustment/interruption compared to those in the imatinib group. Increases in bilirubin and transaminases were commonly reported following Tasigna treatment.
Up to the 48-month cut-off date, three on-treatment deaths have been observed (two in the Tasigna arm and one in the imatinib arm). Three patients died more than 28 days after study drug discontinuation (one in the Tasigna arm and two in the imatinib arm).
QTc intervals >450 ms were observed in 4 patients receiving Tasigna therapy on Day 8. No patient had a QTc interval >480 ms. Increases in QTc interval from baseline of >30 ms were reported for 8 patients (7.9%). No patient experienced QTc prolongation >60 ms in the Tasigna group.
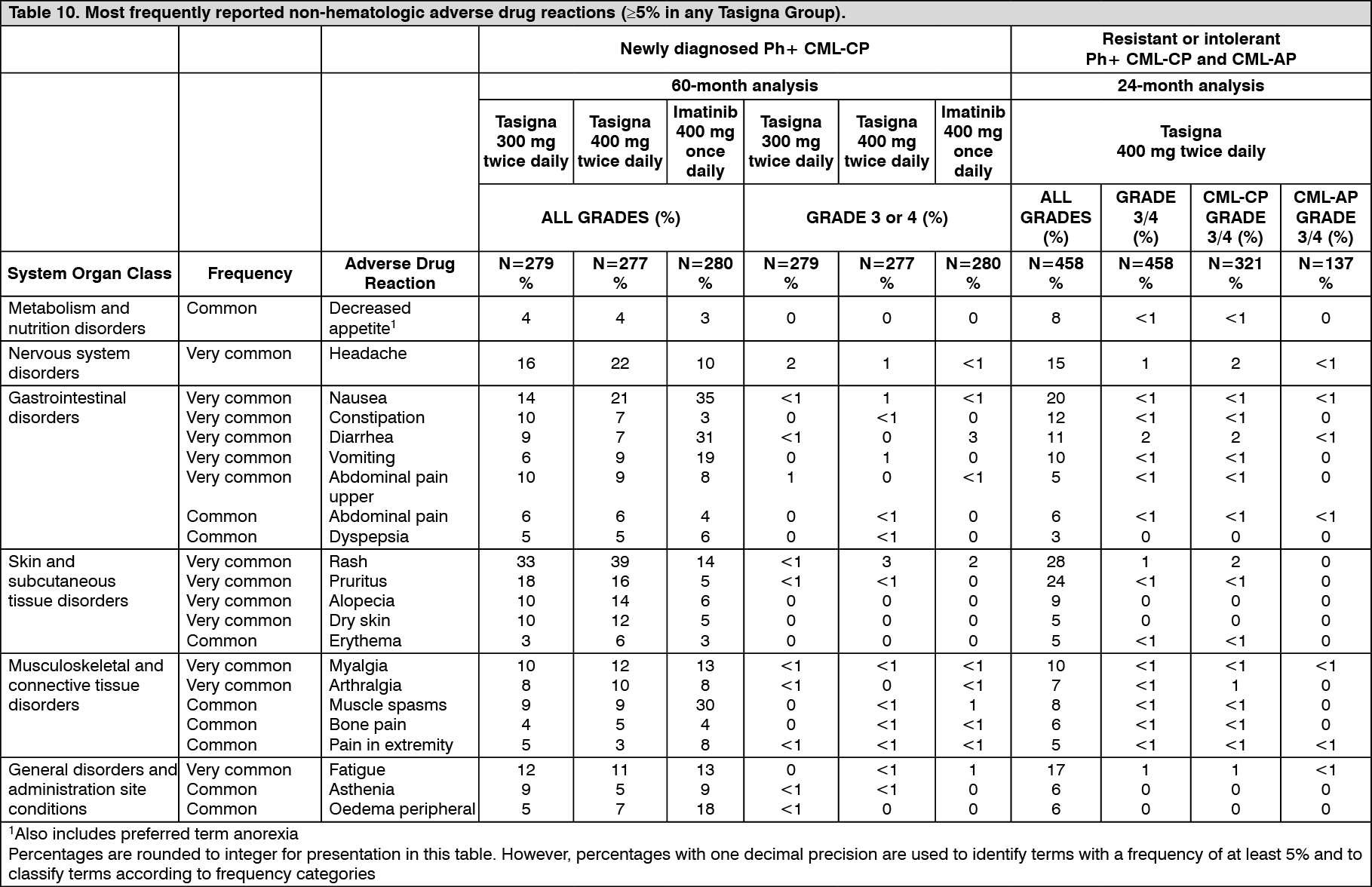
Most frequently reported adverse drug reactions: Non-haematologic ADRs (excluding laboratory abnormalities) that were reported in at least 5% of the adult patients in any of the Tasigna clinical studies that serve as a basis for the listed indications are shown in Table 10. These are ranked under heading of frequency, the most frequent first. Within each frequency grouping adverse drug reactions are presented in order of decreasing seriousness. In addition the corresponding frequency category for each adverse drug reaction is based on the following (CIOMS III) convention: very common (≥1/10) or common (≥1/100 to <1/10). The frequency is based on the highest for any Tasigna group in the two studies, using one decimal precision for percentages. (See Table 10.)
 Click on icon to see table/diagram/image
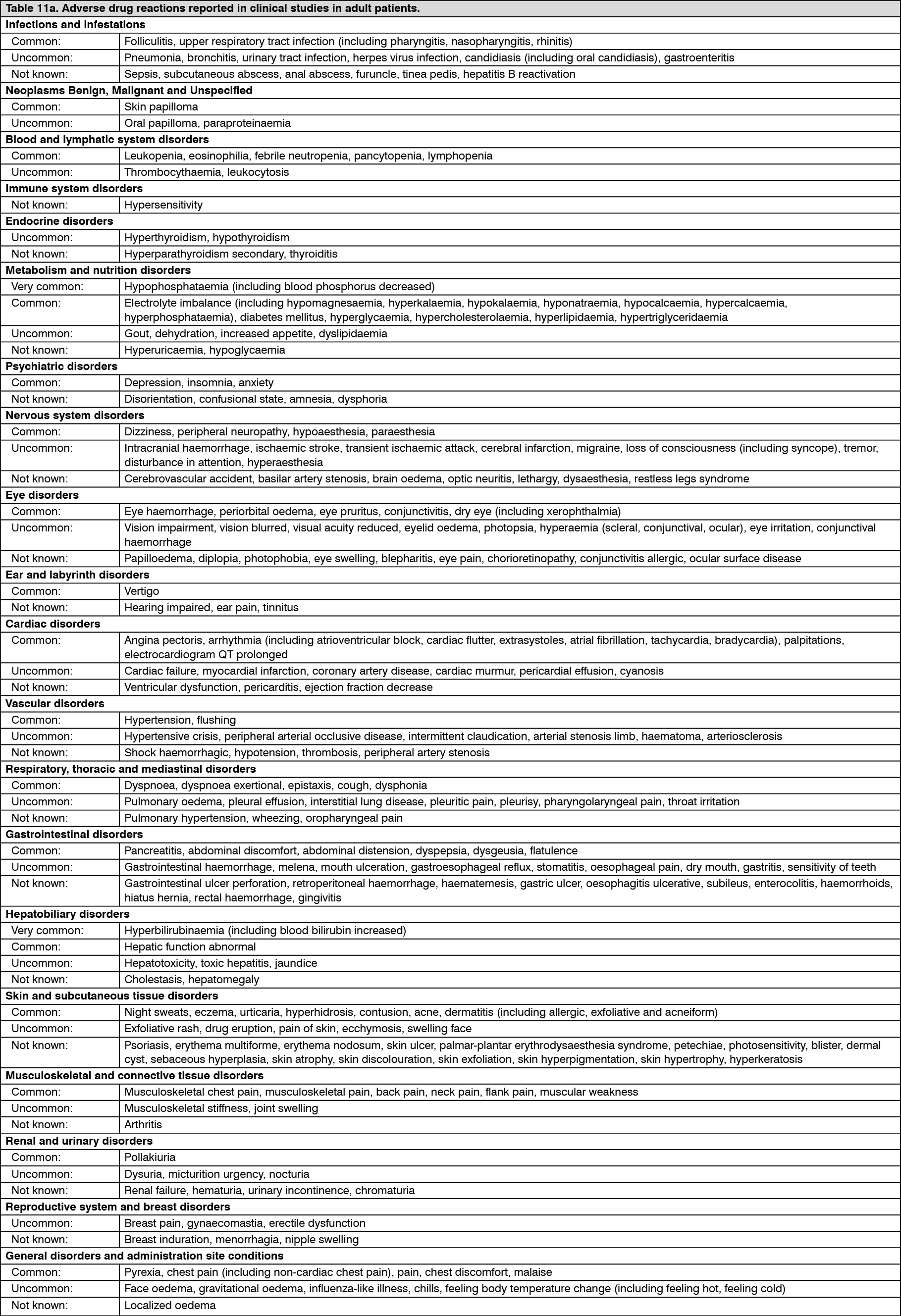
Click on icon to see table/diagram/imageAdditional data from clinical trials: The following adverse drug reactions were reported in adult patients in the Tasigna clinical studies which serve as a basis for the listed indications at the recommended doses at a frequency of less than 5% (common is ≥1/100 to <1/10; uncommon is ≥1/1,000 to <1/100; single events are captured as frequency not known) (Table 11). For laboratory abnormalities, very common events (≥1/10) not included in Table 10 are also reported. These adverse drug reactions are included based on clinical relevance and ranked in decreasing order of seriousness within each category, obtained from two clinical studies: Newly diagnosed Ph+ CML-CP 60 months' analysis and Resistant or intolerant Ph+ CML-CP and CML-AP 24 months' analysis. (See Tables 11a and 11b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
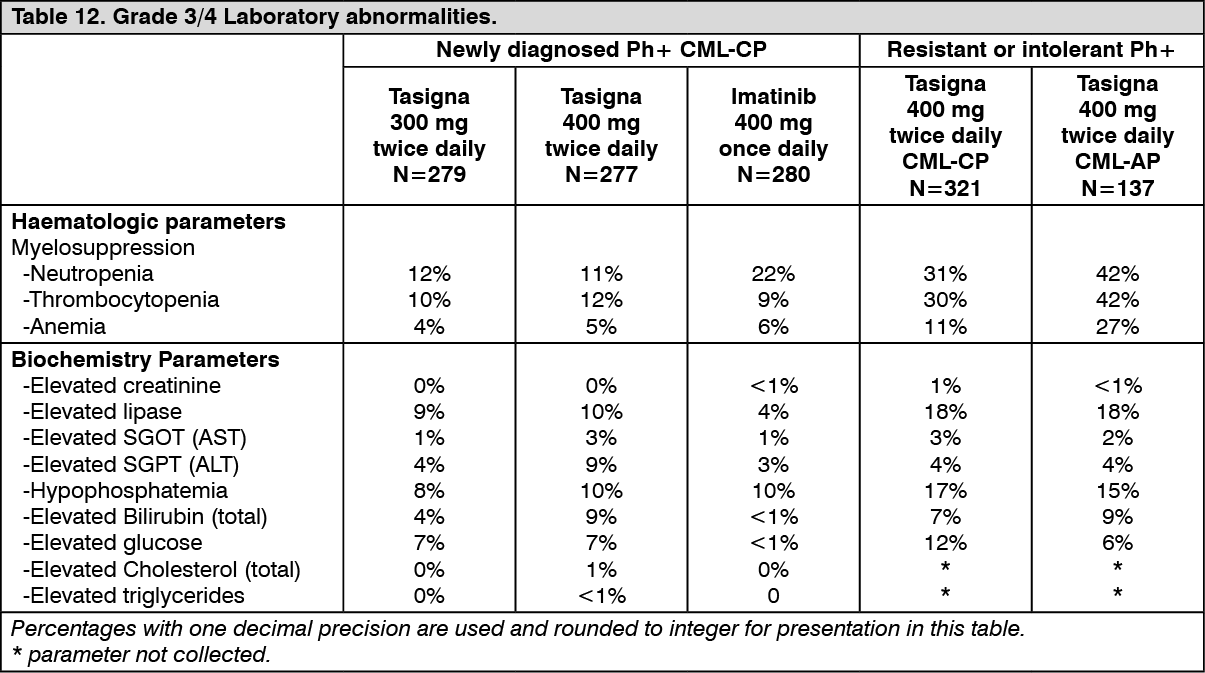
Click on icon to see table/diagram/imageLaboratory abnormalities: Clinically relevant or severe abnormalities of routine haematologic or biochemistry laboratory values in adult patients are presented in Table 12. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment discontinuation in adult Ph+ CML-CP patients who have achieved a sustained deep molecular response: After discontinuation of Tasigna therapy within the framework of attempting treatment-free remission (TFR), patients may experience musculoskeletal symptoms more frequently than before treatment discontinuation, e.g., myalgia, pain in extremity, arthralgia, bone pain, spinal pain, or musculoskeletal pain.
In a Phase II clinical study with newly diagnosed patients with Ph+ CML-CP (N=190), musculoskeletal symptoms within a year of Tasigna discontinuation were reported in 24.7% vs. 16.3% within the previous year on Tasigna treatment.
In a Phase II clinical study with patients with Ph+ CML-CP on Tasigna and previously treated with imatinib (N=126), musculoskeletal symptoms within a year of discontinuation were reported in 42.1% vs. 14.3% within the previous year on Tasigna treatment.
Adverse drug reactions from spontaneous reports and literature cases (frequency not known): The following adverse drug reactions have been derived from post-marketing experience with Tasigna via spontaneous case reports, literature cases, expanded access programs, and clinical studies other than the global registration trials. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to nilotinib exposure.
Frequency not known: Tumour lysis syndrome, facial paralysis.
View ADR Monitoring Form