


 Sign Out
Sign Out

Do not co-administer other medicinal products through the same infusion line.
Substitution by any other biological medicinal product requires the consent of the prescribing physician.
The initial dose of Tecentriq must be administered over 60 minutes. If the first infusion is tolerated, all subsequent infusions may be administered over 30 minutes.
The recommended dose of Tecentriq in monotherapy or combination therapy is 840 mg administered by IV infusion every 2 weeks, or 1200 mg administered by IV infusion every 3 weeks, or 1680 mg administered by IV infusion every 4 weeks.
Tecentriq monotherapy: 1L cisplatin - ineligible mUC, early-stage NSCLC, 1L metastatic NSCLC: Patients should be selected for treatment based on the tumor expression of PD-L1 confirmed by a validated test (see PHARMACOLOGY: Pharmacodynamics: Clinical/Efficacy Studies under Actions).
Tecentriq combination therapy: For the use of Tecentriq in combination therapy, please also refer to the full prescribing information for the combination product. Tecentriq should be administered prior to the combination therapy if given on the same day.
1L non-squamous metastatic NSCLC: Tecentriq in combination with Avastin (bevacizumab), paclitaxel, and carboplatin: During the induction phase, Tecentriq is administered according to its dosing schedule by intravenous (IV) infusion, and Avastin (bevacizumab), paclitaxel, and carboplatin are every 3 weeks for four or six cycles.
The induction phase is followed by a maintenance phase without chemotherapy in which Tecentriq is administered according to its dosing schedule by IV infusion, and Avastin (bevacizumab) is administered every 3 weeks.
Tecentriq in combination with nab-paclitaxel and carboplatin: During the induction phase, Tecentriq is administered according to its dosing schedules by IV infusion, and nab-paclitaxel and carboplatin are administered every 3 weeks for four or six cycles. For each 21-day cycle, nab-paclitaxel and carboplatin are administered on day 1. In addition, nab-paclitaxel is administered on days 8 and 15.
1L ES-SCLC: Tecentriq in combination with carboplatin and etoposide: During the induction phase, Tecentriq is administered according to its dosing schedules by IV infusion and carboplatin and etoposide are administered by IV infusion every three weeks for four cycles. Carboplatin and etoposide are administered on day 1 of each cycle, and etoposide is also administered on days 2 and 3.
1L TNBC: Tecentriq in combination with nab-paclitaxel: Tecentriq is administered according to its dosing schedules by IV infusion and 100 mg/m2 nab-paclitaxel is administered on days 1, 8 and 15 during each 28-day cycle.
Patients should be selected for treatment based on the tumor expression of PD-L1 confirmed by a validated test (see PHARMACOLOGY: Pharmacodynamics: Clinical/Efficacy Studies under Actions).
HCC: Tecentriq in combination with Avastin (bevacizumab): Tecentriq is administered according to its dosing schedules by IV infusion, and Avastin (bevacizumab) 15 mg/kg is administered every 3 weeks.
Duration of treatment: Patients are treated with Tecentriq until loss of clinical benefit (see PHARMACOLOGY: Pharmacodynamics: Clinical/Efficacy Studies under Actions) or unacceptable toxicity.
1L TNBC: Patients are treated with Tecentriq until disease progression or unacceptable toxicity (see PHARMACOLOGY: Pharmacodynamics: Clinical/Efficacy Studies under Actions).
Early-stage NSCLC: Patients are treated with Tecentriq for 1 year unless there is disease recurrence or unacceptable toxicity (see PHARMACOLOGY: Pharmacodynamics: Clinical/Efficacy Studies under Actions).
Delayed or missed doses: If a planned dose of Tecentriq is missed, it should be administered as soon as possible. The schedule of administration should be adjusted to maintain the appropriate interval between doses.
Dose modifications: No dose reductions of Tecentriq are recommended.
Dose modifications for immune-related adverse reactions: Recommendations for specific adverse drug reactions (see General under Precautions and Clinical Trials under Adverse Reactions) are presented in Table 17. (See Table 17.)
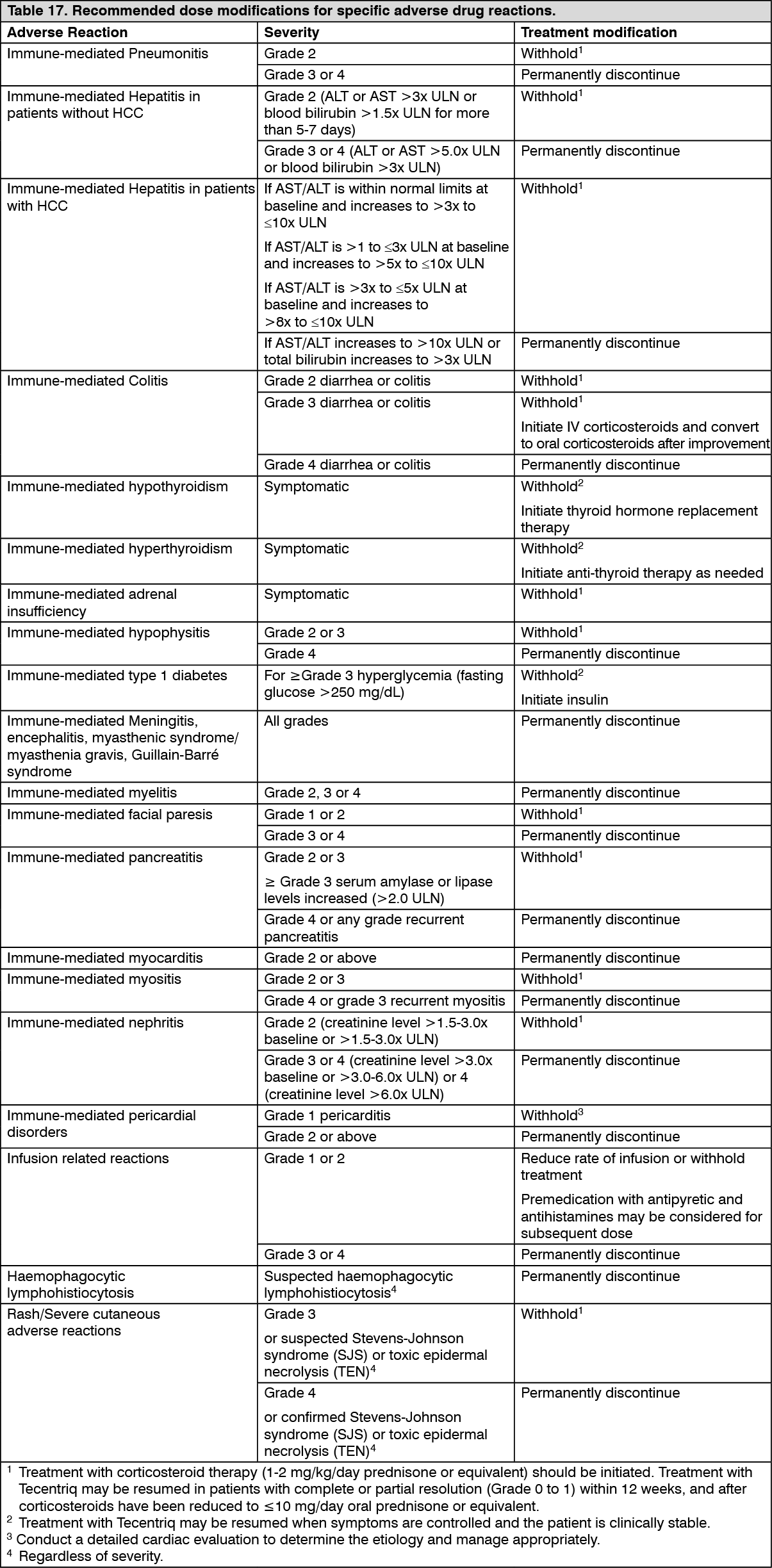 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor other immune-mediated reactions, based on the type and severity of the reaction, treatment with Tecentriq should be withheld for Grades 2 or 3 immune-related adverse reactions and corticosteroid therapy (1-2 mg/kg/day prednisone or equivalent) should be initiated. If symptoms improve to ≤ Grade 1, taper corticosteroids as clinically indicated. Treatment with Tecentriq may be resumed if the event improves to ≤ Grade 1 within 12 weeks, and corticosteroids have been reduced to ≤ 10 mg oral prednisone or equivalent per day.
Treatment with Tecentriq should be permanently discontinued for Grade 4 immune-related adverse reactions, or when unable to reduce corticosteroid dose to the equivalent of ≤ 10 mg prednisone per day within 12 weeks after onset.
Special Dosage Instructions: Pediatric use: The safety and efficacy of Tecentriq in children and adolescents below 18 years of age have not been established (see Use in Children under Precautions and PHARMACOLOGY: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).
Geriatric use: Based on a population pharmacokinetic analysis, no dose adjustment of Tecentriq is required in patients ≥ 65 years of age (see Use in the Elderly under Precautions and PHARMACOLOGY: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).
Renal impairment: Based on a population pharmacokinetic analysis, no dose adjustment is required in patients with renal impairment (see PHARMACOLOGY: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).
Hepatic impairment: Based on a population pharmacokinetic analysis, no dose adjustment is required for patients with mild or moderate hepatic impairment. There are no data on patients with moderate or severe hepatic impairment (see PHARMACOLOGY: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).