Pharmacology: Pharmacodynamics: Mechanism of Action: Thalidomide is an immunomodulatory agent with a spectrum of activity that is not fully characterized. There are many publishes for the studies in anti-inflammatory and anti-immunomodulatory, including inhibition for chemotaxis of neutrophil, decreasing the phagocytosis of monocyte, reducing the production of intermediates of oxygenation (superoxide and hydroxyl radicals), altering the ratio of T-cell (reducing helper T-cell and increasing suppressor T-cell), deducing IgM level and deducing the formation of IgM. Moreover, Administration of thalidomide has been reported to decrease circulating levels of Tumor Necrosis Factor-α (TNF-α) and Interferon-γ (INF- γ), relief the local and systemic symptoms and inhibiting the inflammatory cells in the lesion.
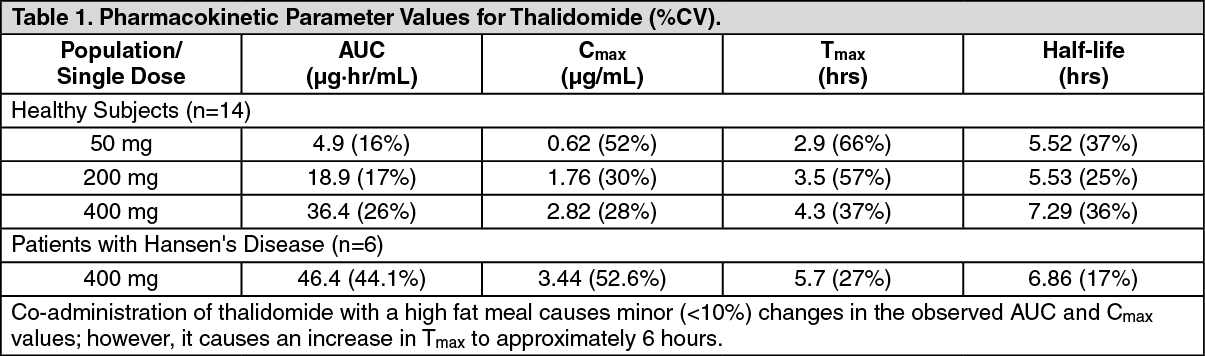
Pharmacokinetics: Absorption: From the other thalidomide products, the mean time to peak plasma concentrations (T
max) is 2.9 to 5.7 hours indicating thalidomide is slowly absorbed from gastrointestinal tract. While the extent of absorption (as measured by area under the curve [AUC]) is proportional to dose in healthy subjects, the observed peak concentration (C
max) increased in a less than proportional manner (see Table 1). This lack of C
max dose proportionality, coupled with the observed increase in T
max values, suggests that the poor solubility of thalidomide in aqueous media may be hindering of absorption. (See Table 1.)
 Click on icon to see table/diagram/image
Distribution:
Click on icon to see table/diagram/image
Distribution: It is not clear whether thalidomide is distributed in the semen.
Metabolism: At the present time, the exact metabolic route and the fate of thalidomide is not known. Thalidomide itself does not appear to be hepatically metabolized to any large extent, but appears to undergo non-enzymatic hydrolysis in plasma to multiple metabolites. In a repeat dose study in which thalidomide 200 mg was administered to 10 healthy females for 18 days, thalidomide displayed similar pharmacokinetic profiles on the first and last day of dosing. This suggests that thalidomide 100 mg/day, thalidomide does not induce or inhibit its own metabolism.
Elimination: As indicated in Table 1, the mean half-life of elimination ranges from approximately 5 to 7 hours following a single dose and is not altered upon multiple dosing. As noted in the metabolism subsection, the precise metabolic fate and route of elimination of thalidomide in humans is not known at this time. Thalidomide itself has a renal clearance of 1.15 mL/minute with less than 0.7% of the dose excreted in the urine as unchanged drug. Following a single dose, urinary levels of thalidomide were undetectable 48 hours after dosing. Although thalidomide is thought to be hydrolyzed to a number of metabolites, only a very small amount (0.02% of the administered dose) of 4-OH-thalidomide was identified in the urine subjects 12 to 24 hours after dosing.
Pharmacokinetic Data in Special Populations: HIV-seropositive Subjects: There is no apparent significant difference in measured pharmacokinetic parameter values between healthy human subjects and HIV-seropositive subjects following single dose administration of thalidomide.
Patients with Hansen's Disease: Analysis of data from a small study in Hansen's patients suggests that these patients, relative to healthy subjects, may have an increased bioavailability of thalidomide. The increase is reflected both in an increased area under the curve and in increased peak plasma levels (see Table 1).
Patients with Renal Insufficiency and/or Hepatic Disease: The pharmacokinetics of thalidomide is patients with renal dysfunction and/or hepatic impairment has not been determined.
Age: Analysis of the data from pharmacokinetic studies ranging in age from 20 to 69 years does not reveal any age-related changes.
Pediatric: No pharmacokinetic studies in subjects below the age of 18 years.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out