


 Sign Out
Sign Out


Adult: Prophylaxis of post operative deep vein thrombosis (DVT) and/or pulmonary embolism (PE): Abdominal surgery: Usual dosage: 4,000 anti-Xa IU (40 mg) once daily by subcutaneous injection, with the initial dose given 2 hours prior to surgery.
Duration of therapy: 7 to 10 days; up to 12 days has been administered in clinical trials.
Hip or knee replacement surgery: Usual dosage: 3,000 anti-Xa IU (30 mg) subcutaneously every 12 hours. Initially given 12 to 24 hours prior to surgery, provided that hemostasis has been established.
Alternative dosage: For hip replacement surgery, 4,000 anti-Xa IU (40 mg) every 24 hours subcutaneously given initially 12 (±3) hours prior to surgery may be considered. Following the initial phase of thromboprophylaxis in hip replacement surgery, continued prophylaxis with enoxaparin 4,000 anti-Xa IU (40 mg) subcutaneously once daily for 3 weeks is recommended.
Duration of therapy: 7 to 10 days; up to 14 days has been administered and well tolerated in clinical trials.
Prophylaxis of deep vein thrombosis (DVT) in medical patients with an acute illness: Usual dosage: 4,000 anti-Xa IU (40 mg) subcutaneously once a day.
Duration of therapy: 6 to 11 days; up to 14 days has been administered and well tolerated in a controlled clinical trial.
Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): Usual dosage: In inpatients treatment with acute DVT with or without PE, 1 mg/kg every 12 hours or 1.5 mg/kg every 24 hours subcutaneously at the same time every day.
In outpatient treatment of patients with acute DVT without PE, 1 mg/kg subcutaneously every 12 hours.
Duration of therapy: Therapy should be continued for a minimum of 5 days and until a therapeutic oral anticoagulant effect has been obtained as indicated by an international normalization ratio (INR) of 2 to 3. The average duration of therapy is 7 days; up to 17 days has been administered and well tolerated in controlled trials.
Concomitant therapy: Warfarin should be initiated when appropriate (usually within 72 hours of enoxaparin).
Prevention of thrombus formation (Clotting) in the extracorporeal circulation during hemodialysis: Usual dosage: 1 mg/kg (100 units/kg) into the arterial line of the circuit at the beginning of the dialysis session. A further dose of 0.5 to 1 mg/kg (50 to 100 units/kg) may be given if required, for example when fibrin rings are found.
The dose should be reduced in patients at high risk of hemorrhage.
Treatment of acute ST-segment elevation myocardial infarction (STEMI): Usual dosage: Single intravenous (IV) bolus of 30 mg plus a 1 mg/kg subcutaneous dose only, followed by 1 mg/kg dosing for the remaining dose subcutaneously every 12 hours.
When administered in conjunction with thrombolytic therapy (fibrin-specific or nonfibrin-specific), enoxaparin should be initiated between 15 minutes before and 30 minutes after the start of thrombolytic therapy.
Maximum dose: 100 mg for the first 2 doses. Only followed by 1 mg/kg dosing for the remaining dose.
Duration of therapy: The American College of Cardiology Foundation/American Heart Association (ACCF/AHA) guidelines recommend continuation for up to 8 days or until revascularization.
Concomitant therapy: Unless contraindicated, all patients should receive aspirin (indefinitely) and clopidogrel.
Percutaneous coronary intervention: If the last subcutaneous administration was given less than 8 hours before balloon inflation, no additional dosing is needed. If the last subcutaneous administration was given more than 8 hours before balloon inflation, an IV bolus of enoxaparin 0.3 mg/kg should be administered.
Prophylaxis of ischemic complications of unstable angina and non-ST elevation myocardial infarction (NSTEMI): Usual dosage: 1 mg/kg subcutaneously every 12 hours.
Duration of therapy: The ACCF/AHA guidelines recommend continuation for the duration of hospitalization (a minimum of at least 2 days) or up to 8 days generally for 2 - 8 days.
Concomitant therapy: Aspirin 100 to 325 mg orally once daily. ACCF/AHA guidelines recommend aspirin doses of 81 mg in preference to higher maintenance doses.
Treatment of ischemic complications of unstable angina and non-ST elevation myocardial infarction (NSTEMI): A dose of 100 anti-Xa IU/kg of enoxaparin is administered by subcutaneous injection twice daily at 12-hour intervals, in combination with aspirin (recommended doses: 75-325 mg orally, following a minimum loading dose of 160 mg). The recommended duration of treatment is about 2-8 days, until the patient is clinically stable.
Pediatric population: The efficacy of enoxaparin in pediatric population has not been established.
Elderly (75 years of age and older): For all therapeutics indication except STEMI, dose reduction is not required in the elderly patients, unless renal function is impaired (see "Renal impairment" as follows).
Acute STEMI - Do not use an initial IV bolus. Initiate dosing with 0.75 mg/kg subcutaneously every 12 hours (maximum, 75 mg for the first 2 doses only, followed by 0.75 mg/kg dosing for the remaining doses).
Hepatic impairment: Enoxaparin has not been studied in patients with hepatic impairment, no dosage adjustments provided. Caution should be used in these patients.
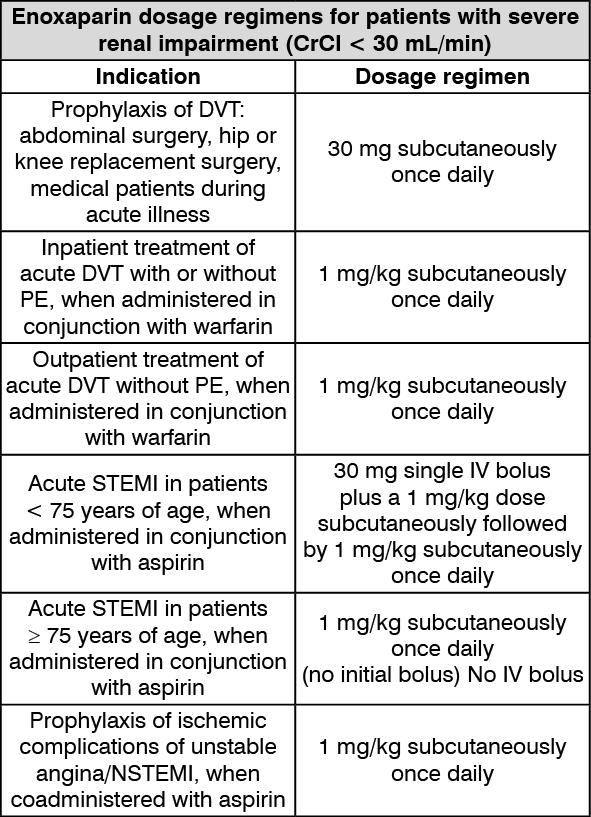
Renal impairment: No dosage adjustment is recommended in patients with mild (creatinine clearance 50 - 80 mL/min) or moderate (creatinine clearance 30 - 50 mL/min) renal impairment. However, dosage should be adjusted in patients with severe renal impairment (creatinine clearance less than 15 - 30 mL/min).
Dose should be adjusted as shown in the table as follows. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMODE OF ADMINISTRATION: Enoxaparin should not be administered by intramuscular (IM) injection. It should be administered by subcutaneous (SC) or intravenous (IV) injection only.
Thenox, in prefilled syringe, are for single, one-time use only.
Subcutaneous injection: Patients should be lying down and enoxaparin should be administered by deep subcutaneous injection. Do not expel the air bubble from the syringe before the injection to avoid the loss of drug when using the 30 and 40 mg prefilled syringes.
Administration should be alternated between the left and the right anterolateral and left and right posterolateral abdominal wall. The whole length of the needle should be introduced into a skin fold held between the thumb and forefinger; the skin fold should be held until the injection is complete. Do not rub the injection site after completion of the injection to minimize bruising.
IV bolus injection: Enoxaparin should be administered through an IV line. It should not be mixed or coadministered with other injection or infusion. To avoid the possible mixture with other drugs, the IV access chosen should be flushed with a sufficient amount of saline or dextrose solution prior to and following the IV bolus administration to clear the port of the drug.
Admixture compatibility: For subcutaneous use, enoxaparin should not be mixed or coadministered with other injections or infusions. For IV use (i.e. for treatment of acute STEMI), enoxaparin can be mixed with normal saline solution (0.9%) or dextrose 5% in water.