


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Pharmacodynamic effects: Natalizumab is a selective adhesion-molecule inhibitor and binds to the α4-subunit of human integrins, which is highly expressed on the surface of all leukocytes, with the exception of neutrophils. Specifically, natalizumab binds to the α4β1 integrin, blocking the interaction with its cognate receptor, vascular cell adhesion molecule-1 (VCAM-1), and ligands osteopontin, and an alternatively spliced domain of fibronectin, connecting segment-1 (CS-1). Natalizumab blocks the interaction of α4β7 integrin with the mucosal addressin cell adhesion molecule-1 (MadCAM-1). Disruption of these molecular interactions prevents transmigration of mononuclear leukocytes across the endothelium into inflamed parenchymal tissue. A further mechanism of action of natalizumab may be to suppress ongoing inflammatory reactions in diseased tissues by inhibiting the interaction of α4-expressing leukocytes with their ligands in the extracellular matrix and on parenchymal cells. As such, natalizumab may act to suppress inflammatory activity present at the disease site, and inhibit further recruitment of immune cells into inflamed tissues.
In MS, lesions are believed to occur when activated T-lymphocytes cross the blood brain barrier (BBB). Leukocyte migration across the BBB involves interaction between adhesion molecules on inflammatory cells and endothelial cells of the vessel wall. The interaction between α4β1 and its targets is an important component of pathological inflammation in the brain and disruption of these interactions leads to reduced inflammation. Under normal conditions, VCAM-1 is not expressed in the brain parenchyma. However, in the presence of pro inflammatory cytokines, VCAM-1 is upregulated on endothelial cells and possibly on glial cells near the sites of inflammation. In the setting of central nervous system (CNS) inflammation in MS, it is the interaction of α4β1 with VCAM-1, CS-1 and osteopontin that mediates the firm adhesion and transmigration of leukocytes into the brain parenchyma and may perpetuate the inflammatory cascade in CNS tissue. Blockade of the molecular interactions of α4β1 with its targets reduces inflammatory activity present in the brain in MS and inhibits further recruitment of immune cells into inflamed tissue, thus reducing the formation or enlargement of MS lesions.
Clinical Efficacy: Efficacy as monotherapy has been evaluated in one randomised, double-blind, placebo controlled study lasting 2 years (AFFIRM study) in relapsing remitting MS patients who had experienced at least 1 clinical relapse during the year prior to entry and had a Kurtzke Expanded Disability Status Scale (EDSS) score between 0 and 5. Median age was 37 years, with a median disease duration of 5 years. The patients were randomised with a 2:1 ratio to receive TYSABRI 300 mg (n = 627) or placebo (n = 315) every 4 weeks for up to 30 infusions. Neurological evaluations were performed every 12 weeks and at times of suspected relapse. MRI evaluations for T1-weighted gadolinium (Gd)-enhancing lesions and T2-hyperintense lesions were performed annually.
Study features and results are presented in Table 1. (See Table 1.)
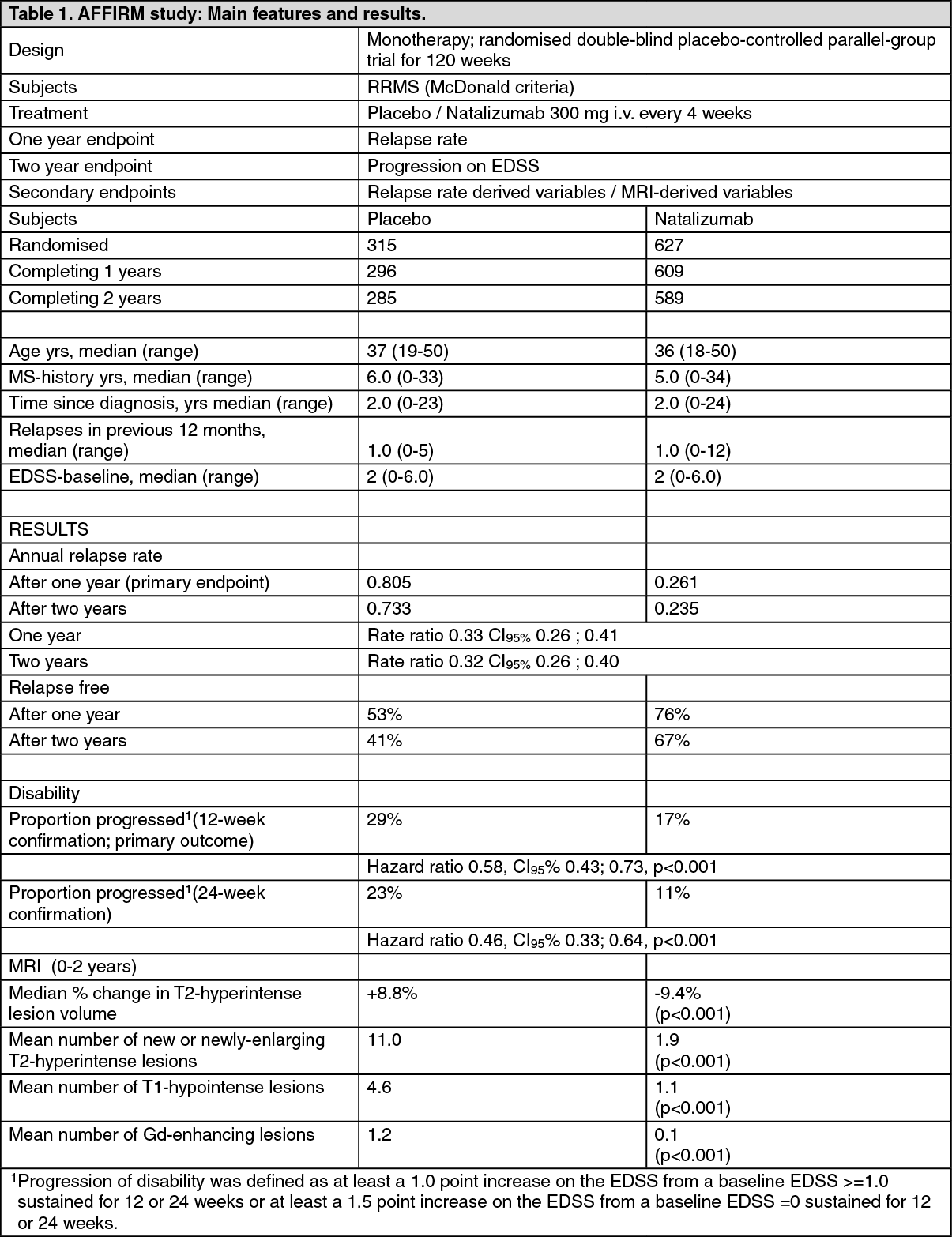 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the sub-group of patients indicated for treatment of rapidly evolving relapsing remitting MS (patients with 2 or more relapses and 1 or more Gd+ lesion), the annualised relapse rate was 0.282 in the TYSABRI treated group (n = 148) and 1.455 in the placebo group (n = 61) (p <0.001). Hazard ratio for disability progression was 0.36 (95% CI : 0.17, 0.76) p = 0.008. These results were obtained from a post hoc analysis and should be interpreted cautiously. No information on the severity of the relapses before inclusion of patients in the study is available.
Interim analysis of results (as of May 2015) from the ongoing TYSABRI Observational Program (TOP), a phase 4, multicentre, single-arm study (n=5770) demonstrated that patients switching from beta interferon (n= 3255) or glatiramer acetate (n= 1384) to TYSABRI showed a sustained, significant decrease in annualised relapse rate (p< 0.0001). Mean EDSS scores remained stable over 5 years. Consistent with efficacy results observed for patients switching from beta interferon or glatiramer acetate to TYSABRI, for patients switching from fingolimod (n=147) to TYSABRI, a significant decrease in annualised relapse rate (ARR) was observed, which remained stable over 2 years, and mean EDSS scores remained similar from baseline to Year 2. The limited sample size and shorter duration of TYSABRI exposure for this subgroup of patients should be considered when interpreting these data.
A post-marketing meta-analysis was conducted using data from 621 paediatric MS patients treated with TYSABRI (median age 17 years, range was 7-18 years, 91% aged ≥14 years). Within this analysis, a limited subset of patients with data available prior to treatment (158 of the 621 patients) demonstrated a reduction in ARR from 1.466 (95% CI 1.337, 1.604) prior to treatment to 0.110 (95% CI 0.094, 0.128).
Pharmacokinetics: Following the repeat intravenous administration of a 300 mg dose of natalizumab to MS patients, the mean maximum observed serum concentration was 110 ± 52 μg/ml. Mean average steady-state trough natalizumab concentrations over the dosing period ranged from 23 μg/ml to 29 μg/ml. The predicted time to steady-state was approximately 36 weeks.
A population pharmacokinetics analysis was conducted on samples from over 1,100 MS patients receiving doses ranging from 3 to 6 mg/kg natalizumab. Of these, 581 patients received a fixed 300 mg dose as monotherapy. The mean ± SD steady state clearance was 13.1 ± 5.0 ml/h, with a mean ± SD half life of 16 ± 4 days. The analysis explored the effects of selected covariates including body weight, age, gender, hepatic and renal function, and presence of anti-natalizumab antibodies upon pharmacokinetics. Only body weight and the presence of anti-natalizumab antibodies were found to influence natalizumab disposition. Body weight was found to influence clearance in a less-than-proportional manner, such that a 43% change in body weight resulted in a 31% to 34% change in clearance. The change in clearance was not clinically significant. The presence of persistent anti-natalizumab antibodies increased natalizumab clearance approximately 3-fold, consistent with reduced serum natalizumab concentrations observed in persistently antibody-positive patients, (see Adverse Reactions).
The pharmacokinetics of natalizumab in paediatric MS patients has not been established. The pharmacokinetics of natalizumab in patients with renal or hepatic insufficiency has not been studied.
The effect of plasma exchange on natalizumab clearance and pharmacodynamics was evaluated in a study of 12 MS patients. Estimates of the total natalizumab removal after 3 plasma exchanges (over a 5-8 day interval) was approximately 70-80%. This compares to approximately 40% seen in earlier studies in which measurements occurred after natalizumab discontinuation over a similar period of observation. The impact of plasma exchange on the restitution of lymphocyte migration and ultimately its clinical usefulness is unknown.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity and genotoxicity.
Consistent with the pharmacological activity of natalizumab, altered trafficking of lymphocytes was seen as white blood cell increases as well as increased spleen weights in most in vivo studies. These changes were reversible and did not appear to have any adverse toxicological consequences.
In studies conducted in mice, growth and metastasis of melanoma and lymphoblastic leukaemia tumour cells was not increased by the administration of natalizumab.
No clastogenic or mutagenic effects of natalizumab were observed in the Ames or human chromosomal aberration assays. Natalizumab showed no effects on in vitro assays of α4-integrin-positive tumour line proliferation or cytotoxicity.
Reductions in female guinea pig fertility were observed in one study at doses in excess of the human dose; natalizumab did not affect male fertility.
The effect of natalizumab on reproduction was evaluated in 5 studies, 3 in guinea pigs and 2 in cynomolgus monkeys. These studies showed no evidence of teratogenic effects or effects on growth of offspring. In one study in guinea pigs, a small reduction in pup survival was noted. In a study in monkeys, the number of abortions was doubled in the natalizumab 30 mg/kg treatment groups versus matching control groups. This was the result of a high incidence of abortions in treated groups in the first cohort that was not observed in the second cohort. No effects on abortion rates were noted in any other study. A study in pregnant cynomolgus monkeys demonstrated natalizumab-related changes in the foetus that included mild anaemia, reduced platelet counts, increased spleen weights and reduced liver and thymus weights. These changes were associated with increased splenic extramedullary haematopoiesis, thymic atrophy and decreased hepatic haematopoiesis. Platelet counts were also reduced in offspring born to mothers treated with natalizumab until parturition, however there was no evidence of anaemia in these offspring. All changes were observed at doses in excess of the human dose and were reversed upon clearance of natalizumab.
In cynomolgus monkeys treated with natalizumab until parturition, low levels of natalizumab were detected in the breast milk of some animals.