Each capsule contains ursodeoxycholic acid (ursodiol) 250 mg.
Pharmacodynamics: Mechanism of Action: Anticholelithic: Although the exact mechanism of ursodiol's anticholelithic action is not completely understood, it is known that when administered orally ursodiol is concentrated in bile and decreases biliary cholesterol saturation by suppressing hepatic synthesis and secretion of cholesterol, and by inhibiting its intestinal absorption. The reduced cholesterol saturation permits the gradual solubilization of cholesterol from gallstones, resulting in their eventual dissolution.
Ursodiol increases bile flow. In chronic cholestatic liver disease, ursodiol appears to reduce the
detergent properties of the bile salts, thus reducing their cytotoxicity. Also, ursodiol may protect liver cells from the damaging activity of toxic bile acids (e.g., lithocholate, deoxycholate, and chenodeoxycholate), which increase in concentration in patients with chronic liver disease.
Pharmacokinetics: Absorption: About 90% of an oral dose is absorbed in small intestine.
Only small amounts of ursodiol appear in the systemic circulation.
Distribution: Following absorption from the GI tract, ursodiol distributes to the portal vein and undergoes hepatic extraction (about 50% in the absence of liver disease; extent of extraction decreases as severity of liver disease increases) from portal blood by the liver (i.e., there is a large first-pass effect). After the drug is conjugated in the liver, it is distributed into the bile.
Ursodiol in the bile is concentrated in the gallbladder and distributed into the duodenum in gallbladder bile via the cystic and common ducts by gallbladder contractions stimulated by physiologic responses to eating.
During chronic administration (13-15 mg/kg daily), ursodiol becomes a major biliary and plasma bile acid, comprising 30-50% of biliary and plasma bile acids. Following discontinuance of the drug, the concentration of ursodiol in the bile falls exponentially.
It is not known whether ursodiol is distributed into milk.
Plasma Protein Binding: Healthy individuals: ≥ 70% (as unconjugated ursodiol).
Healthy individuals or patients with primary biliary cirrhosis: Extent of protein binding of conjugated ursodiol is not known.
Metabolism: Ursodiol is conjugated with glycine or taurine in the liver and distributed into the bile. Ursodiol conjugates are absorbed into the small intestine by passive and active mechanisms. These conjugates may be deconjugated in the ileum by intestinal enzymes (or by bacteria in the small intestine), creating free ursodiol that can be reabsorbed and reconjugated in the liver.
Unabsorbed ursodiol reaches the colon unchanged, where it is primarily 7-dehydroxylated to form lithocholic acid. Some ursodiol may be epimerized to form chenodiol, which also undergoes 7-dehydroxylation to form lithocholic acid.
A small portion of lithocholic acid is reabsorbed and conjugated in the liver with glycine or taurine, and sulfated at the 3 position. Ursodiol also can be oxidized at the 7-carbon, producing 7-keto-lithocholic acid. Absorbed 7-keto-lithocholic acid is stereospecifically reduced in the liver to chenodiol. A small portion of orally administered ursodiol undergoes bacterial degradation with each cycle of enterohepatic circulation.
Elimination: Ursodiol is excreted principally in the feces. Urinary excretion increases with treatment but remains below 1% except in patients with severe cholestatic liver disease.
Half-life: About 4-6 days.
Gallstone Dissolution: Ursodiol capsules are used for dissolution of gallstones in patients with radiolucent, noncalcified gallbladder stones <20 mm in greatest diameter who are not candidates for cholecystectomy because of systemic disease, advanced age, idiosyncratic reaction to general anesthesia, or refusal of surgery; considered pharmacologic treatment of choice in these patients.
Dissolution of gallstones usually requires several months of ursodiol therapy. Complete dissolution of gallstones does not occur in all patients, and recurrence, which may occur within 5 years, is reported in up to 50% of patients who have achieved dissolution of the stones with the drug. Monitor for recurrence of stones.
Successful dissolution of gallstones with ursodiol occurs rarely in patients with calcified gallstones prior to treatment, those who develop stone calcification or gallbladder nonvisualization during treatment, and those with gallstones >20 mm in greatest diameter.
Successful dissolution is more likely in patients with floating or floatable stones (i.e., those with high cholesterol content) and dissolution is inversely related to stone size for stones <20 mm in greatest diameter.
Gallbladder nonvisualization prior to treatment is not a contraindication to ursodiol therapy; however, discontinue treatment in patients who develop gallbladder nonvisualization during therapy since this is predictive of failure for complete dissolution.
Prevention of Gallstones: Ursodiol capsules are used for prevention of gallstone formation in obese patients undergoing rapid weight loss.
Primary Biliary Cirrhosis.
Recommended Dose: General dosing considerations: Gallstone dissolution: Obtain ultrasound images of the gallbladder at 6 - month intervals for the first year of ursodiol therapy to monitor gallstone response. If gallstones appear to have dissolved, continue ursodiol therapy and confirm dissolution on a repeat ultrasound examination within 1 to 3 months. Most patients who eventually achieve complete stone dissolution will show partial or complete dissolution at the first on - treatment reevaluation. If partial stone dissolution is not seen by 12 months of ursodiol therapy, the likelihood of success is greatly reduced.
Safety of use beyond 24 months of therapy has not been established.
Adults: Gallstone dissolution: 8 to 10 mg/kg/day given in 2 or 3 divided doses.
Gallstone prevention: 600 mg/day (300 mg twice daily) in patients undergoing rapid weight loss.
Primary biliary cirrhosis: 10-15 mg/kg/day in 2-4 divided doses with food.
Adjust dosage regimen according to patient's response and tolerance.
Special Populations: Renal function impairment: No specific dosage recommendations at this time.
Hepatic function impairment: No specific dosage recommendations at this time.
Geriatric patients: Select dosage with caution.
Mode of Administration: Administer orally.
Overdose: Doses of ursodiol in the range of 16 to 20 mg/kg/day have been tolerated by 7 patients for 6 to 37 months without symptoms. The LD50 for ursodiol in rats is over 5000 mg/kg given over 7 to 10 days and over 7500 mg/kg for mice.
Single oral doses of ursodiol at 10, 5 and 10 g/kg in mice, rat and dogs, respectively, were not lethal. A single oral dose of ursodiol at 1.5 g/kg was lethal in hamsters. Symptoms of acute toxicity were salivation and vomiting in dogs and ataxia, dyspnea, ptosis, agonal convulsions and coma in hamsters.
Treatment: The most likely manifestation of severe overdose with ursodiol would likely be diarrhea, which should be treated symptomatically.
Hypersensitivity or intolerance to ursodiol or any of the components of the formulations.
Ursodiol will not dissolve calcified cholesterol stones, radiopaque stones or radiolucent bile pigment stones. Hence, patients with such stones are not candidates for ursodiol therapy.
Patients with compelling reasons for cholecystectomy including unremitting acute cholecystitis, cholangitis, biliary obstruction, gallstone pancreatitis or biliary GI fistula are not candidates for ursodiol therapy.
Allergy to bile acids.
Monitoring: Abnormalities in liver enzymes have not been associated with ursodiol therapy and in fact, ursodiol has been shown to decrease liver enzyme levels in liver disease. However, patients given with ursodiol should have AST and ALT measured at the initiation of therapy and thereafter as indicated by the particular clinical circumstances.
Patients with variceal bleeding, hepatic encephalopathy, ascites or in need of an urgent liver transplant should receive appropriate specific treatment.
Hepatic effects: Ursodiol therapy has not been associated with liver damage. Lithocholic acid, a naturally occurring bile acid, is known to be a liver - toxic metabolite. This bile acid is formed in the gut from ursodiol less efficiently and in smaller amounts than that seen from chenodiol. Lithocholic acid is detoxified in the liver by sulfation and although man appears to be an efficient sulfater, it is possible that some patients may have a congenital or acquired deficiency in sulfation, thereby predisposing them to lithocholate-induced liver damage.
Use in Children: The safety and effectiveness of ursodiol in pediatric patients have not been established.
Pregnancy: Pregnancy risk factor B.
There have been no adequate and well-controlled studies of the use of ursodiol in pregnant woman, but inadvertent exposure of 4 women to therapeutic doses of the drug in the first trimester of pregnancy during the ursodiol trials led to no evidence of effects on the fetus or newborn baby. Although it seems unlikely, the possibility that ursodiol can cause fetal harm cannot be ruled out; hence, the drug is not recommended for use during pregnancy.
Lactation: It is not known whether ursodiol is excreted in human milk. Because many drugs are excreted in human milk, exercise caution when ursodiol is administered to a breastfeeding mother.
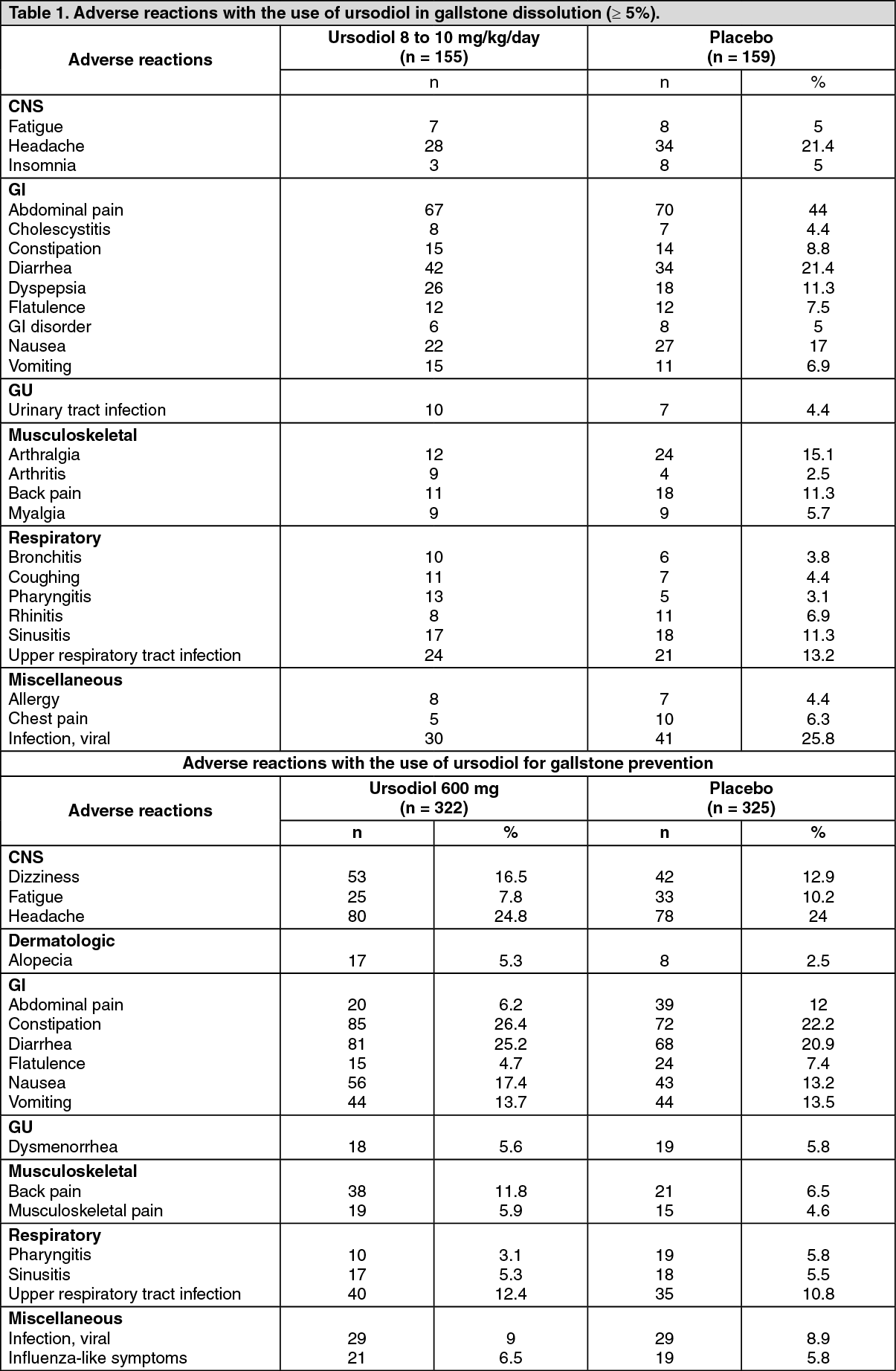
See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
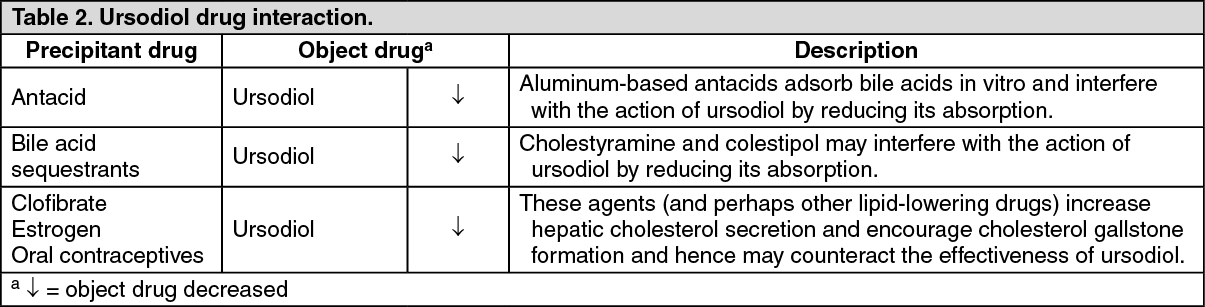
See Table 2.
Click on icon to see table/diagram/image
Store below 30°C. Protect from moisture.
A05AA02 - ursodeoxycholic acid ; Belongs to the class of bile acids. Used in bile therapy.
Ursolin cap 250 mg
10 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out