Antihemorrhagics: Blood Coagulation Factor VIII.
ATC code: B02BD02.
Pharmacology: Mechanism of Action: XYNTHA temporarily replaces the missing clotting factor VIII that is needed for effective hemostasis.
Pharmacodynamics: The activated partial thromboplastin time (aPTT) is prolonged in patients with hemophilia. Determination of aPTT is a conventional
in vitro assay for biological activity of factor VIII. Treatment with XYNTHA normalizes the aPTT over the effective dosing period.
Clinical studies: Three completed multicenter, open-label studies support the analysis of safety and efficacy of XYNTHA in on-demand treatment and control of bleeding episodes and perioperative management, and routine prophylaxis in PTPs with hemophilia A. These completed clinical studies for XYNTHA examined 174 PTP subjects, 94 from the first study, and 50 from a second study, for on-demand treatment and routine prophylaxis and 30 from a third study for surgical prophylaxis. Subjects with severe to moderately severe hemophilia A (FVIII:C ≤2%) and no history of FVIII inhibitors were eligible for the trials.
On-demand Treatment and Control of Bleeding Episodes: On-demand treatment in adolescents and adults: Ninety-four (94) subjects, 12 years of age and older received XYNTHA in a routine prophylaxis treatment regimen with on-demand treatment administered as clinically indicated. All 94 subjects were treated with at least one dose and all are included in the intent-to-treat (ITT) population. Eighty-nine (89) subjects accrued ≥50 EDs. Median age for the 94 treated subjects was 24 years (mean 28 and min-max: 12-60 years).
Of these 94 subjects, 30 evaluable subjects participated in a randomized crossover pharmacokinetics sub-study. Twenty-five (25/30) of these subjects with FVIII:C ≤1% completed both the first (PK1) and the second (PK2) pharmacokinetic assessments (see Pharmacokinetics as follows).
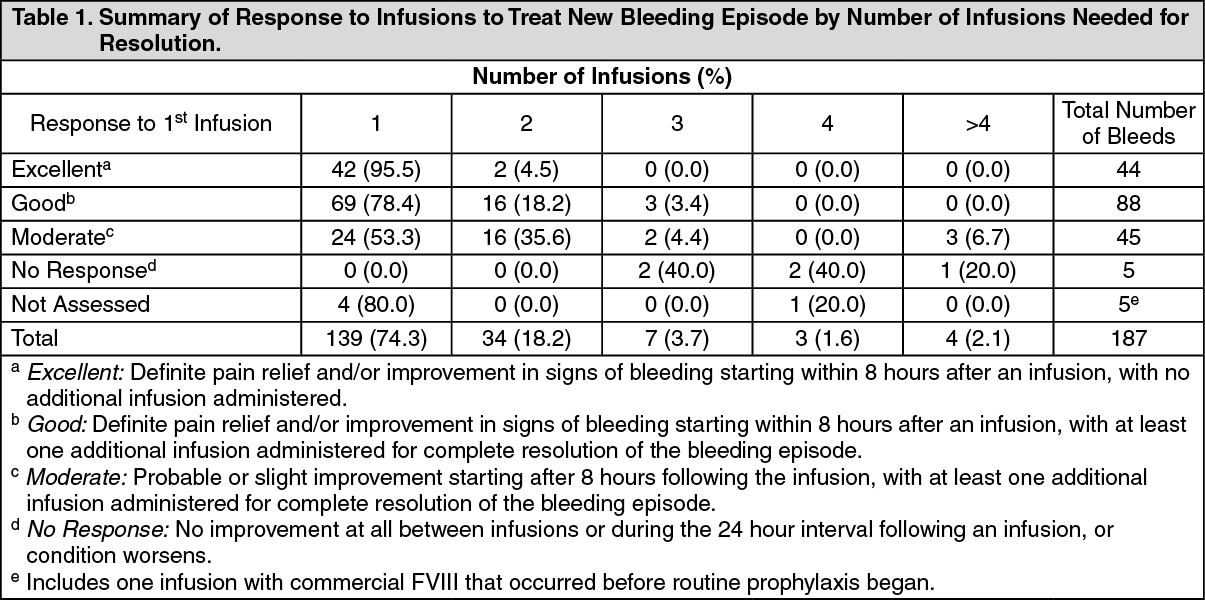
Fifty-three subjects (53/94) received XYNTHA on-demand treatment for a total of 187 bleeding episodes. Seven of these bleeding episodes occurred in subjects prior to switching to a prophylaxis treatment regimen. One hundred ten of 180 bleeds (110/180 or 61%) occurred ≤48 hours after the last dose and 39% (70/180 bleeds) occurred >48 hours after the last dose. The majority of bleeds reported to occur ≤48 hours after the last prophylaxis dose were traumatic (64/110 bleeds or 58%). Forty-two bleeds (42/70 or 60%) reported to occur >48 hours after the last prophylaxis dose were spontaneous. The on-demand treatment dosing regimen was determined by the investigator. The median dose for on-demand treatment was 31 IU/kg (min-max: 6-74 IU/kg) and the median exposure per subject was 3 days (min-max: 1-26).
The majority of bleeding episodes (173/187 or 93%) resolved with 1 or 2 infusions (Table 1). One hundred thirty-two of 187 bleeding episodes (132/187 or 71%) treated with XYNTHA were rated excellent or good in their response to initial treatment, 45 (24%) were rated moderate. Five (3%) were rated no response, and 5 (3%) were not rated. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Of the 94 subjects described as previously mentioned, in the first completed open-label safety and efficacy study of XYNTHA, 18 were adolescent subjects 12 to <17 years of age with severe to moderately severe hemophilia A (FVIII:C ≤2%). Ten (10) of these adolescent subjects, received XYNTHA for the on-demand treatment of 66 bleeding episodes, with the majority of the bleeding episodes (63/66 or 95%) resolving with 1 or 2 infusions. The response to infusion was rated on a pre-specified 4 point hemostatic efficacy scale. Thirty-eight (38) of 66 bleeding episodes (58%) were rated excellent or good in their response to initial treatment, 24 (36%) were rated as moderate, and 4 (6%) were not rated. The median dose per on demand infusion was 47 IU/kg (min-max: 24-74).
On-demand treatment in children: Additional data for 50 subjects are available from a second safety and efficacy study of XYNTHA in children (≤12 years of age) with severe to moderately severe hemophilia A (FVIII:C ≤2%). Of the 50 subjects, 38 subjects received XYNTHA for on-demand and follow-up treatment of 562 bleeding episodes with the majority of the bleeding episodes (518/562 or 92%) resolving with 1 or 2 infusions. Of 559 bleeding episodes treated with XYNTHA with response assessments to the first infusion, 526 (94%) were rated excellent or good in their response to initial treatment and 27 (5%) were rated as moderate. The median dose per on-demand infusion was 28 IU/kg (min-max: 10-92).
Perioperative Management: In a study (n=30) for surgical prophylaxis in subjects with hemophilia A, XYNTHA was administered to 25 efficacy-evaluable PTPs undergoing major surgical procedures (11 total knee replacements, 1 hip replacement, 5 synovectomies, 1 left ulnar nerve transposition release, 1 ventral hernia repair/scar revision, 1 knee arthroscopy, 1 revision and debridement of the knee after a total knee replacement, 1 hip arthroplasty revision, 1 stapes replacement, 1 ankle arthrodesis, and 1 pseudotumor excision).
The results of the hemostatic efficacy ratings for these subjects are presented in Table 2. Investigator's ratings of efficacy at the end of surgery and at the end of the initial postoperative period were excellent or good for all assessments. Intraoperative blood loss was reported as "normal" or "absent" for all subjects. Thirteen of the subjects (13/25 or 52%) had blood loss in the postoperative period. The postoperative blood loss was rated as "normal" for ten of these cases while three cases were rated "abnormal" (1 due to hemorrhage following surgical trauma to the epigastric artery, 1 due to an 800 mL blood loss after hip replacement surgery, and 1 after an elbow synovectomy where the blood loss could not be measured by the investigator). (See Table 2.)
Click on icon to see table/diagram/image
Routine Prophylaxis: One hundred and two (102) subjects (94 subjects ≥12 years of age and 8 subjects <12 years of age) received XYNTHA for routine prophylaxis, for comparison of annualized bleeding rate (ABR) to on-demand treatment alone as a part of 2 completed studies. XYNTHA was administered for routine prophylaxis at a dose of 25 ± 5 IU/kg every other day (in subjects <12 years of age) or 30 ± 5 IU/kg administered 3 times weekly (in subjects 12 years of age or older), with provisions for dose escalation based on pre-specified criteria (over a 4-week period, 2 spontaneous bleeds into a major joint and/or target joint, or 3 or more spontaneous bleeding episodes in any location). Among these 102 subjects, 7 dose escalations were prescribed for 6 subjects.
In subjects ≥12 years, 42 subjects (42/94 or 45%) reported no bleeding while on routine prophylaxis. The mean±SD total ABR during routine prophylaxis was 4.0±6.64 with median (min-max) of 1.9 (0.0-44.2). The mean ABR for subjects during routine prophylaxis was 88% lower than the mean ABR for subjects during on-demand treatment (Table 3).
In subjects <12 years, 4 subjects (4/8 or 50%) reported no bleeding while on routine prophylaxis. The mean±SD total ABR during routine prophylaxis was 1.5±2.2 with median (min-max) of 0.6 (0.0-6.2). The mean ABR for subjects during routine prophylaxis was 97% lower than the mean ABR for subjects during on-demand treatment (see Table 3).
Click on icon to see table/diagram/image
Pediatric Use: Safety and efficacy with XYNTHA were evaluated in clinical studies in 68 pediatric subjects <17 years of age (18 subjects aged 12 to <17 years, 50 subjects aged ≤12 years). There were no apparent differences in the efficacy and safety in pediatric subjects as compared to adults (see Adverse Reactions).
In comparison to the pharmacokinetic parameters reported in adults, children have shorter half-lives, larger volumes of distribution and lower recovery of factor VIII after XYNTHA administration. The clearance (based on per kg body weight) is approximately 40% higher in children. Higher or more frequent doses may be required to account for the observed differences in pharmacokinetic parameters (see Pharmacokinetics as follows).
Pharmacokinetics: The pharmacokinetic parameters of XYNTHA in 30 PTPs 12 to 60 years old, who received a single infusion of 50 IU/kg XYNTHA are summarized in Table 4.
In addition, 25 of the same subjects later received a single infusion of 50 IU/kg of XYNTHA for a 6-month follow-up pharmacokinetic study. The parameters were comparable between baseline and 6 months, indicating no time-dependent changes in the pharmacokinetics of XYNTHA.
In a separate study, 8 of 30 subjects at least 12 years old with hemophilia A undergoing elective major surgery received a single 50 IU/kg infusion of XYNTHA. The pharmacokinetic parameters in these subjects are also summarized in Table 4. (See Table 4.)
Click on icon to see table/diagram/image
Table 5 shows the pharmacokinetic parameters of nine children; four aged 14 or 15 years of age, who are also included in the summary for the adults as previously mentioned, along with five children aged 3.7-5.8 years after single 50 IU/kg doses of XYNTHA. Compared to adults, the half-life of XYNTHA is shorter in children and the clearance (based on per kg body weight) is approximately 40% higher in children. (See Table 5.)
Click on icon to see table/diagram/image
Geriatric Use: Clinical studies of XYNTHA did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy.
Toxicology: Preclinical safety data: Carcinogenesis, Mutagenesis, Impairment of Fertility: No studies have been conducted with XYNTHA to assess its mutagenic or carcinogenic potential. XYNTHA has been shown to be comparable to the predecessor product with respect to its biochemical and physicochemical properties, as well as its nonclinical
in vivo pharmacology and toxicology. By inference, predecessor product and XYNTHA would be expected to have equivalent mutagenic and carcinogenic potential. The predecessor product has been shown to be nongenotoxic in the mouse micronucleus assay. No studies have been conducted in animals to assess impairment of fertility or fetal development.
Animal Toxicology and/or Pharmacology: Preclinical studies evaluating XYNTHA in hemophilia A dogs without inhibitors demonstrated safe and effective restoration of hemostasis. XYNTHA demonstrated a toxicological profile that was similar to the toxicological profile observed with the predecessor product. Toxicity associated with XYNTHA was primarily associated with anti-FVIII neutralizing antibody generation first detectable at 15 days of repeat dosing in high (approximately 735 IU/kg/day) level-dosed, non-human primates.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image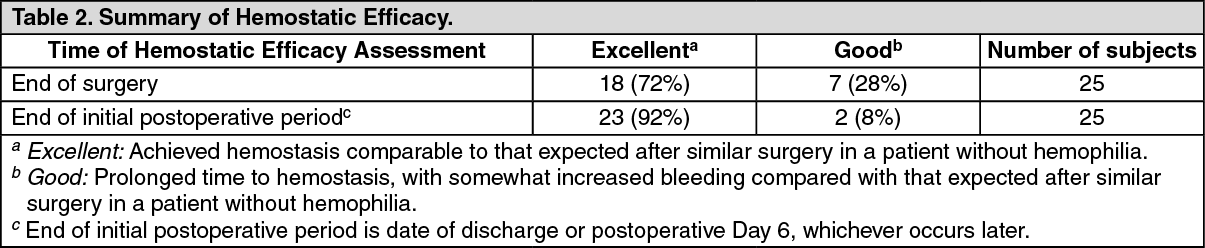 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image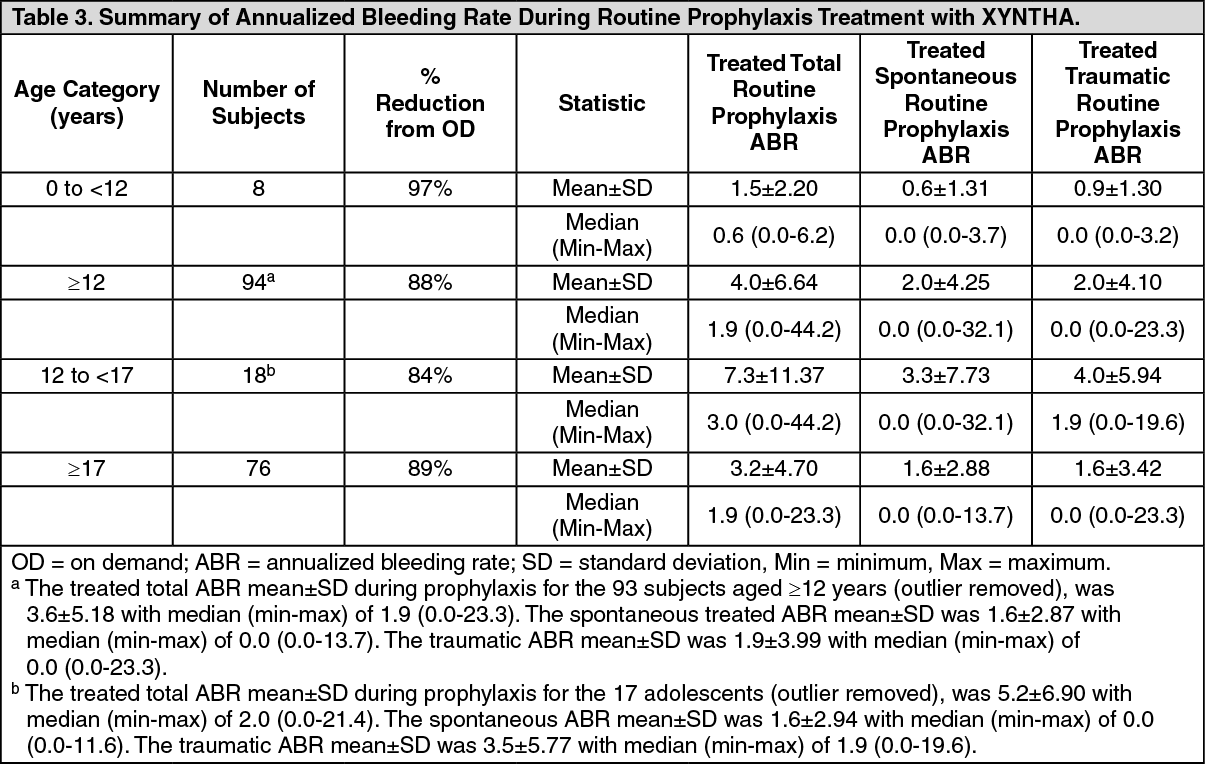 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image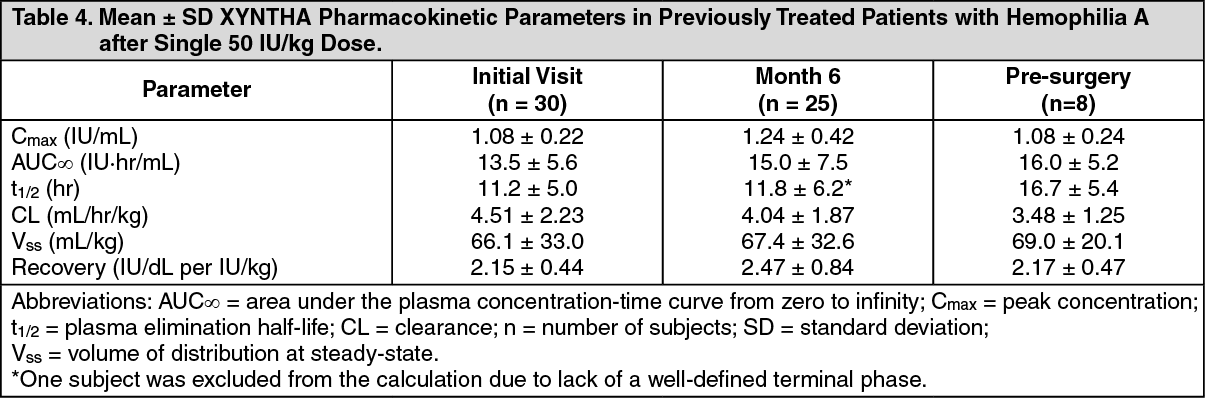 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image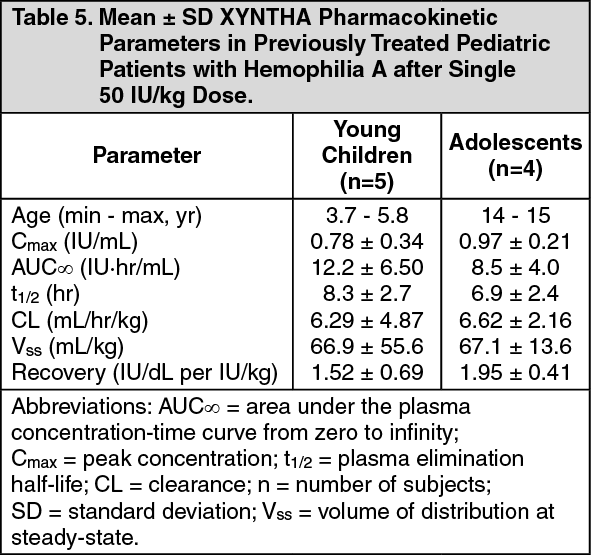 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image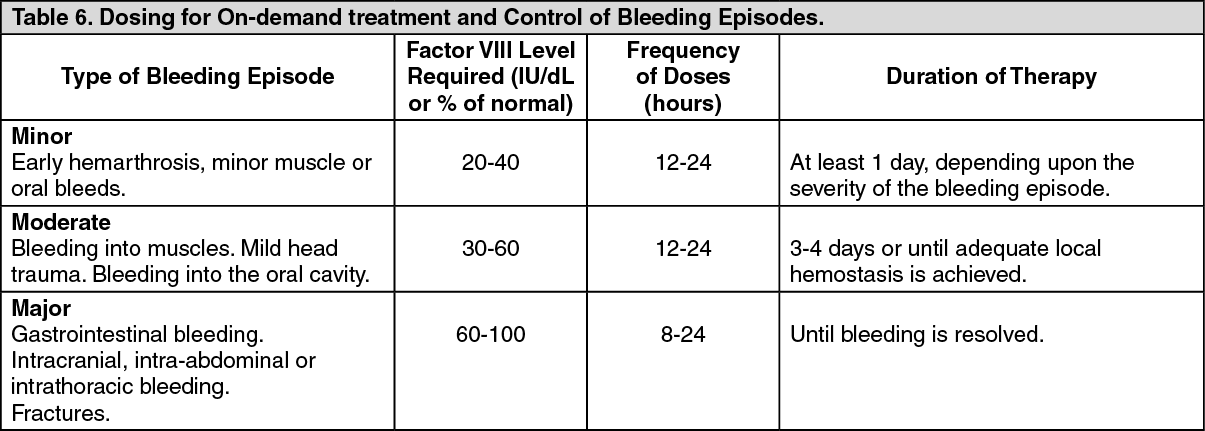 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image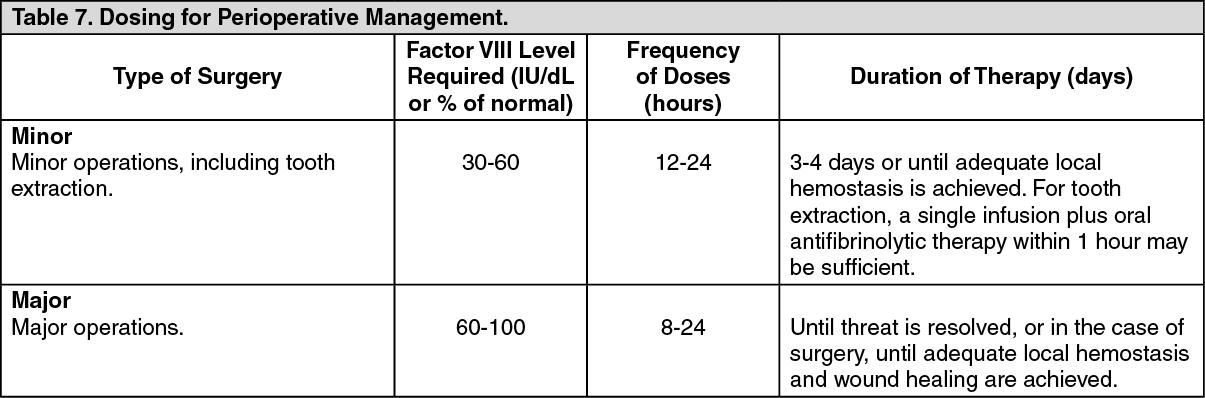 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
