


 Sign Out
Sign Out
Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described as follows reflect exposure to AVELOX in 14981 patients in 71 active controlled Phase II-IV clinical trials in different indications (see Indications/Uses). The population studied had a mean age of 50 years (approximately 73% of the population was less than 65 years of age), 50% were male, 63% were Caucasian, 12% were Asian and 9% were Black. Patients received AVELOX 400 mg once daily oral, intravenous, or sequentially (intravenous followed by oral). Treatment duration was usually 6 to 10 days, and the mean number of days on therapy was 9 days.
Discontinuation of AVELOX due to adverse reactions occurred in 5% of patients overall, 4% of patients treated with 400 mg PO, 4% with 400 mg intravenous and 8% with sequential therapy 400 mg oral/intravenous. The most common adverse reactions (>0.3%) leading to discontinuation with the 400 mg oral doses were nausea, diarrhea, dizziness, and vomiting. The most common adverse reaction leading to discontinuation with the 400 mg intravenous dose was rash. The most common adverse reactions leading to discontinuation with the 400 mg intravenous/oral sequential dose were diarrhea, pyrexia.
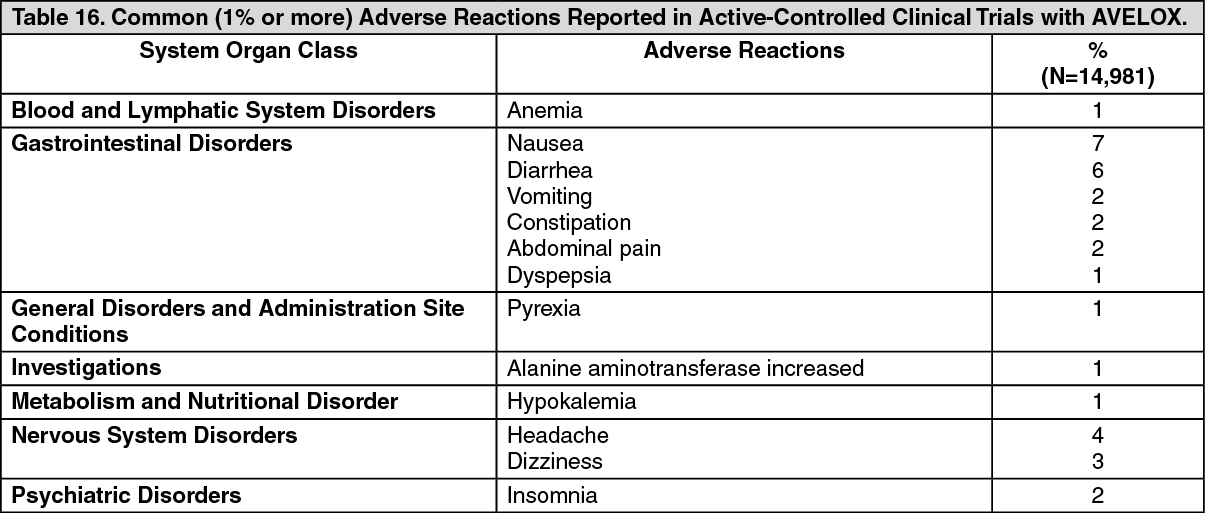
Adverse reactions occurring in 1% of AVELOX-treated patients and less common adverse reactions, occurring in 0.1 to 1% of AVELOX-treated patients, are shown in Table 16 and Table 17, respectively. The most common adverse drug reactions (3%) are nausea, diarrhea, headache, and dizziness. (See Tables 16 and 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image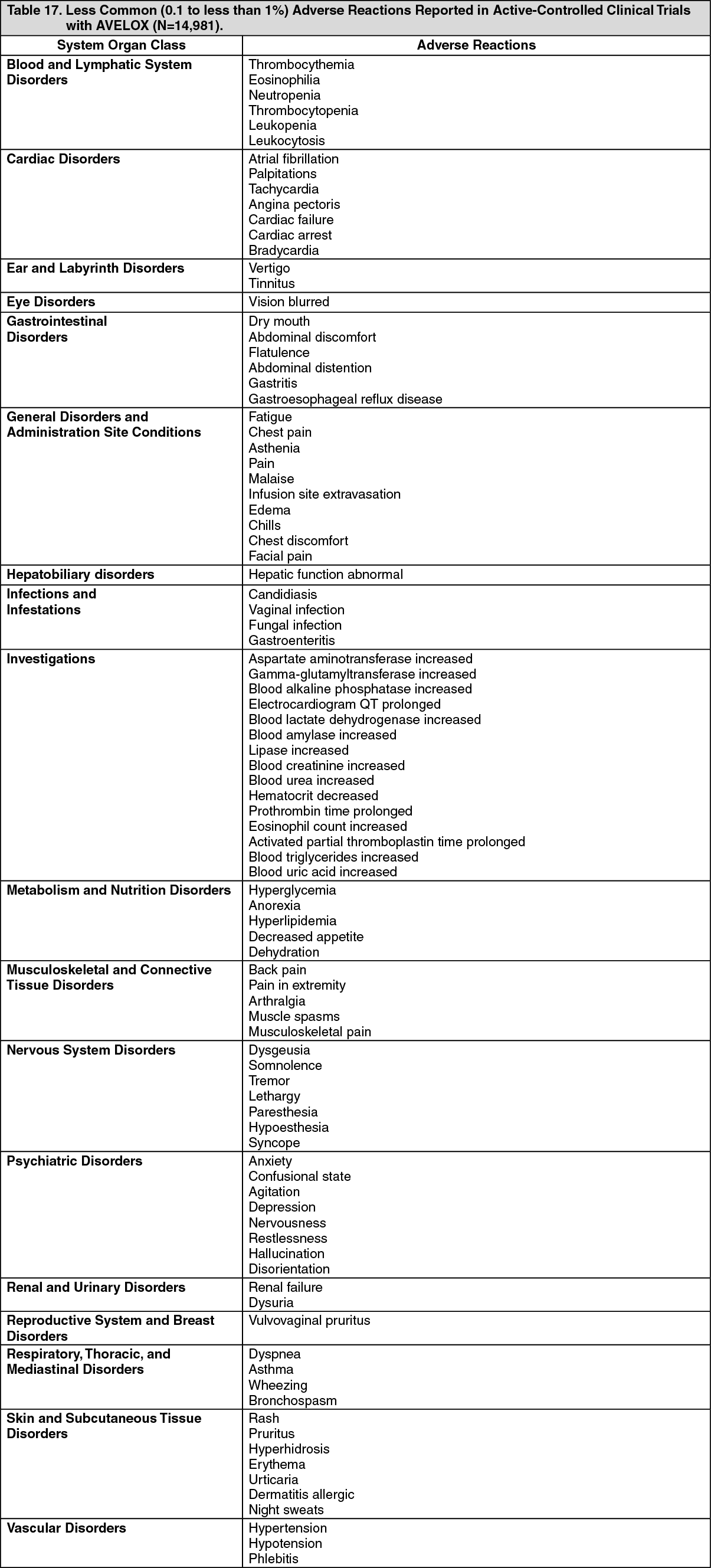 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther undesirable effects: For oral formulations: Cardiovascular system disorders: Common (1 to less than 10%): QT prolongation in patients with hypokalaemia.
Uncommon (0.1% to less than 1%): QT prolongation.
Rare (0.01 to less than 0.1%): ventricular tachyarrhythmias, syncope (i.e., acute and short lasting loss of consciousness).
Very rare (less than 0.01%): Unspecified arrhythmias, torsade de pointes, cardiac arrest.
For i.v. formulations of moxifloxacin: The following undesirable effects have a higher frequency category in the subgroup of IV treated patients with or without subsequent oral therapy.
Uncommon: ventricular tachyarrhythmias.
Laboratory Changes: Changes in laboratory parameters, which are not listed above and which occurred in 2% or more of patients and at an incidence greater than in controls included: increases in mean corpuscular hemoglobin (MCH), neutrophils, white blood cells (WBCs), prothrombin time (PT) ratio, ionized calcium, chloride, albumin, globulin, bilirubin; decreases in hemoglobin, red blood cells (RBCs), neutrophils, eosinophils, basophils, glucose, oxygen partial pressure (pO2), bilirubin, and amylase. It cannot be determined if any of the above laboratory abnormalities were caused by the drug or the underlying condition being treated.
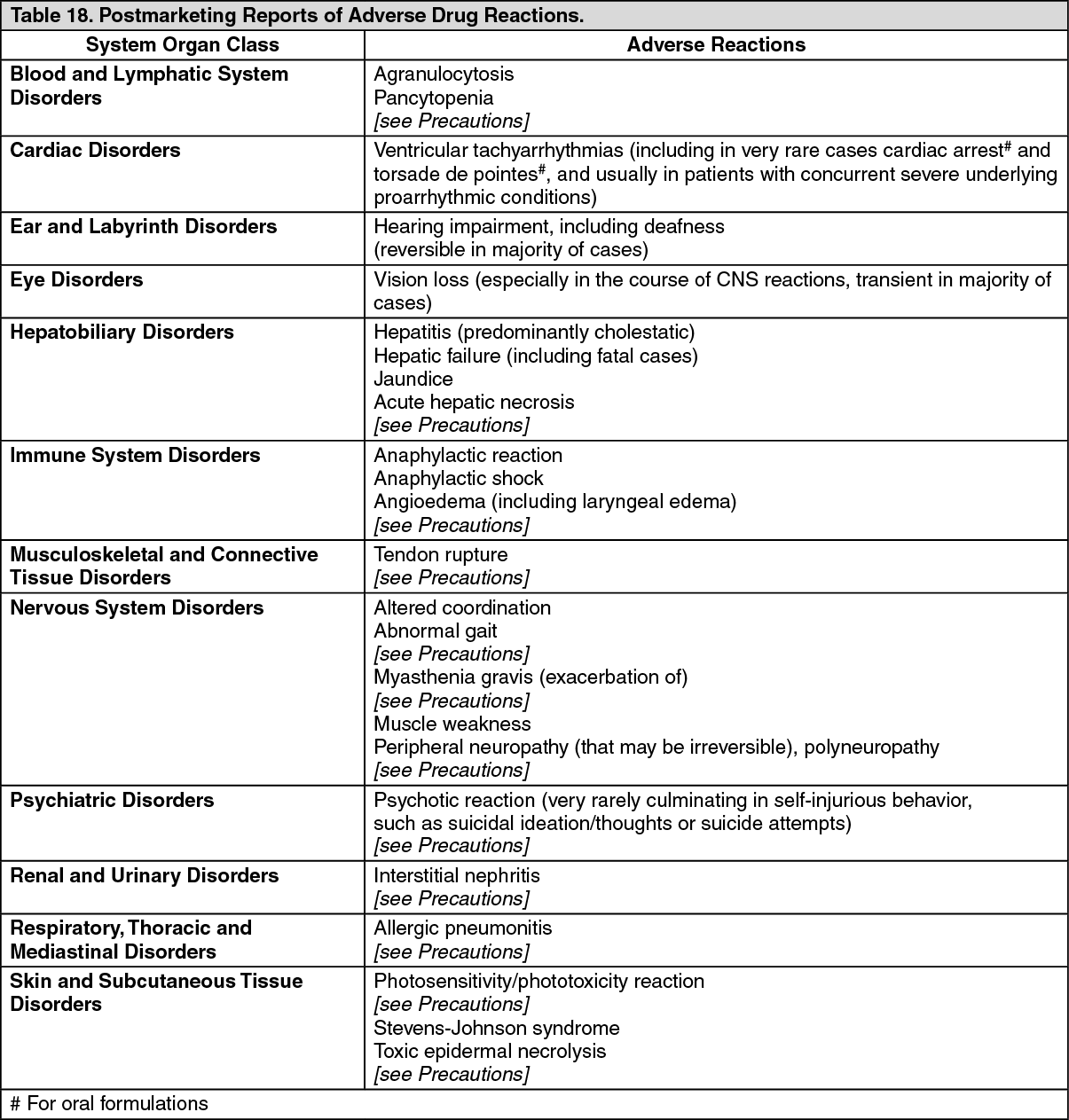
Postmarketing Experience: Table 18 as follows lists adverse reactions that have been identified during post-approval use of AVELOX. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. (See Table 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form