


 Sign Out
Sign Out
Discontinue AVELOX immediately at the first signs or symptoms of any serious adverse reaction. In addition, avoid the use of fluoroquinolones, including AVELOX, in patients who have experienced any of these serious adverse reactions associated with fluoroquinolones.
Tendinitis and Tendon Rupture: Fluoroquinolones, including AVELOX, have been associated with an increased risk of tendinitis and tendon rupture in all ages (see Precautions and Adverse Reactions). This adverse reaction most frequently involves the Achilles tendon, and has also been reported with the rotator cuff (the shoulder), the hand, the biceps, the thumb, and other tendons. Tendinitis or tendon rupture can occur within hours or days of starting moxifloxacin or as long as several months after completion of therapy. Tendinitis and tendon rupture can occur bilaterally.
The risk of developing fluoroquinolone-associated tendinitis and tendon rupture is increased in patients over 60 years of age, in patients taking corticosteroid drugs, and in patients with kidney, heart or lung transplants. Other factors that may independently increase the risk of tendon rupture include strenuous physical activity, renal failure, and previous tendon disorders such as rheumatoid arthritis. Tendinitis and tendon rupture have also occurred in patients taking fluoroquinolones who do not have the above risk factors. Discontinue AVELOX immediately if the patient experiences pain, swelling, inflammation or rupture of a tendon. Patients should be advised to rest at the first sign of tendinitis or tendon rupture, and to contact their doctor regarding changing to a non-quinolone antimicrobial drug. Avoid fluoroquinolones, including AVELOX, in patients who have a history of tendon disorders or who have experienced tendinitis or tendon rupture (see Adverse Reactions).
Peripheral Neuropathy: Fluoroquinolones, including AVELOX, have been associated with an increased risk of peripheral neuropathy. Cases of sensory or sensorimotor axonal polyneuropathy affecting small and/or large axons resulting in paresthesias, hypoesthesias, dysesthesias and weakness have been reported in patients receiving fluoroquinolones including AVELOX. Symptoms may occur soon after initiation of AVELOX and may be irreversible in some patients (see Precautions and Adverse Reactions).
Discontinue AVELOX immediately if the patient experiences symptoms of peripheral neuropathy including pain, burning, tingling, numbness, and/or weakness or other alterations of sensation including light touch, pain, temperature, position sense, and vibratory sensation. Avoid fluoroquinolones, including AVELOX, in patients who have previously experienced peripheral neuropathy.
Central Nervous System Effects: Psychiatric Adverse Reactions: Fluoroquinolones, including AVELOX, have been associated with an increased risk of psychiatric adverse reactions, including: toxic psychosis, hallucinations, or paranoia; depression or suicidal thoughts or acts; anxiety, agitation, or nervousness; confusion, delirium, disorientation, or disturbances in attention; insomnia or nightmares; memory impairment. These adverse reactions may occur following the first dose. If these reactions occur in patients receiving AVELOX, discontinue AVELOX immediately and institute appropriate measures (see Adverse Reactions).
Central Nervous System Adverse Reactions: Fluoroquinolones, including AVELOX, have been associated with an increased risk of seizures (convulsions), increased intracranial pressure (including pseudotumor cerebri), dizziness, and tremors. As with all fluoroquinolones, use AVELOX with caution in patients with known or suspected CNS disorders (for example, severe cerebral arteriosclerosis, epilepsy) or in the presence of other risk factors that may predispose to seizures or lower the seizure threshold. These adverse reactions may occur following the first dose. If these reactions occur in patient receiving AVELOX, discontinue AVELOX immediately and institute appropriate measures (see Interactions and Adverse Reactions).
Exacerbation of Myasthenia Gravis: Fluoroquinolones, including AVELOX, have neuromuscular blocking activity and may exacerbate muscle weakness in patients with myasthenia gravis. Postmarketing serious adverse reactions, including deaths and requirement for ventilatory support, have been associated with fluoroquinolone use in patients with myasthenia gravis. Avoid AVELOX in patients with known history of myasthenia gravis.
Prolongation of QTc interval and potentially QTc-prolongation related clinical conditions: For oral formulations: Moxifloxacin has been shown to prolong the QTc interval of the electrocardiogram in some patients. In the analysis of ECGs obtained in the clinical trial program, QTc prolongation with moxifloxacin was 6 msec ± 26 msec, 1.4% compared to baseline. As women tend to have a longer baseline QTc interval compared with men, they may be more sensitive to QTc-prolonging medications. Elderly patients may also be more susceptible to drug-associated effects on the QT interval.
Medication that can reduce potassium levels should be used with caution in patients receiving moxifloxacin.
Moxifloxacin should be used with caution in patients with ongoing proarrhythmic conditions (especially women and elderly patients), such as acute myocardial ischaemia or QT prolongation as this may lead to an increased risk for ventricular arrhythmias (incl. torsade de pointes) and cardiac arrest (see also Contraindications). The magnitude of QT prolongation may increase with increasing concentrations of the drug. Therefore, the recommended dose should not be exceeded.
The benefit of moxifloxacin treatment especially in infections with a low degree of severity should be balanced with the information contained in the warnings and precautions section. If signs of cardiac arrhythmia occur during treatment with moxifloxacin, treatment should be stopped and an ECG should be performed.
For i.v. formulations: Moxifloxacin has been shown to prolong the QTc interval on the electrocardiogram in some patients. The magnitude of QT prolongation may increase with increasing plasma concentrations due to rapid intravenous infusion. Therefore, the duration of infusion should not be less than the recommended 60 minutes and the intravenous dose of 400 mg once a day should not be exceed. For more details see as follows and refer to Contraindications and Interactions.
Treatment with moxifloxacin should be stopped if signs or symptoms that may be associated with cardiac arrhythmia occur during treatment, with or without ECG findings.
Moxifloxacin should be used with caution in patients with any condition pre-disposing to cardiac arrhythmias (e.g. acute myocardial ischemia) because they may have an increased risk of developing ventricular arrhythmias (incl. torsade de pointes) and cardiac arrest. See also Contraindications and Interactions. Moxifloxacin should be used with caution in patients who are taking medication that can reduce potassium levels. See also Contraindications.
Moxifloxacin should be used with caution in patients who are taking medications associated with clinically significant bradycardia. See also Contraindications.
Female patients and elderly patients may be more sensitive to the effects of QTc-prolonging medications such as moxifloxacin and therefore special caution is required.
Avoid AVELOX in patients with the following risk factors due to the lack of clinical experience with the drug in these patient populations: Known prolongation of the QT interval; Ventricular arrhythmias including torsade de pointes because QT prolongation may lead to an increased risk for these conditions; Ongoing proarrhythmic conditions, such as clinically significant bradycardia and acute myocardial ischemia; Uncorrected hypokalemia or hypomagnesemia; Class IA (for example, quinidine, procainamide) or Class III (for example, amiodarone, sotalol) antiarrhythmic agents; Other drugs that prolong the QT interval such as cisapride, erythromycin, antipsychotics, and tricyclic antidepressants.
Elderly patients using intravenous AVELOX may be more susceptible to drug-associated QT prolongation (see Use in Elderly as follows).
In patients with mild, moderate, or severe liver cirrhosis, metabolic disturbances associated with hepatic insufficiency may lead to QT prolongation. Monitor ECG in patients with liver cirrhosis treated with AVELOX (see Pharmacology: Pharmacokinetics under Actions).
The magnitude of QT prolongation may increase with increasing concentrations of the drug or increasing rates of infusion of the intravenous formulation. Therefore the recommended dose or infusion rate should not be exceeded.
In premarketing clinical trials, the rate of cardiovascular adverse reactions was similar in 798 AVELOX and 702 comparator treated patients who received concomitant therapy with drugs known to prolong the QTc interval. No excess in cardiovascular morbidity or mortality attributable to QTc prolongation occurred with AVELOX treatment in over 15,500 patients in controlled clinical studies, including 759 patients who were hypokalemic at the start of treatment, and there was no increase in mortality in over 18,000 AVELOX tablet treated patients in a postmarketing observational study in which ECGs were not performed.
Other Serious and Sometimes Fatal Adverse Reactions: Other serious and sometimes fatal adverse reactions, some due to hypersensitivity, and some due to uncertain etiology, have been reported in patients receiving therapy with fluoroquinolones, including AVELOX. These reactions may be severe and generally occur following the administration of multiple doses. Clinical manifestations may include one or more of the following: Fever, rash, or severe dermatologic reactions (for example, toxic epidermal necrolysis, Stevens-Johnson syndrome); Vasculitis, arthralgia, myalgia, serum sickness; Allergic pneumonitis; Interstitial nephritis, acute renal insufficiency or failure; Hepatitis, jaundice, acute hepatic necrosis or failure; Anemia, including hemolytic and aplastic, thrombocytopenia, including thrombotic thrombocytopenic purpura, leukopenia, agranulocytosis, pancytopenia, and/or other hematologic abnormalities.
Discontinue AVELOX immediately at the first appearance of a skin rash, jaundice, or any other sign of hypersensitivity and institute supportive measures.
Cases of fulminant hepatitis potentially leading to liver failure (including fatal cases) have been reported with AVELOX (see Adverse Reactions). Patients should be advised to contact their doctor immediately prior to continuing treatment if symptoms of liver failure occur.
Hypersensitivity Reactions: Serious anaphylactic reactions, some following the first dose, have been reported in patients receiving fluoroquinolone therapy, including AVELOX. Some reactions were accompanied by cardiovascular collapse, loss of consciousness, tingling, pharyngeal or facial edema, dyspnea, urticaria, and itching. Discontinue AVELOX at the first appearance of a skin rash or any other sign of hypersensitivity (see Precautions).
Risk of Aortic Aneurysm and Dissection: Epidemiologic studies report an increased rate of aortic aneurysm and dissection within two months following use of fluoroquinolones, particularly in elderly patients. The cause for the increased risk has not been identified. In patients with a known aortic aneurysm or patients who are at greater risk for aortic aneurysms, reserve AVELOX for use only when there are no alternative antibacterial treatments available.
Therefore, fluoroquinolones should only be used after careful benefit-risk assessment and after consideration of other therapeutic options in patients with positive family history of aneurysm disease, or in patients diagnosed with pre-existing aortic aneurysm and/or aortic dissection, or in presence of other risk factors or conditions predisposing for aortic aneurysm and dissection (e.g., Marfan syndrome, vascular Ehlers-Danlos syndrome, Takayasu arteritis, giant cell arteritis, Behcet's disease, hypertension, known atherosclerosis).
In case of sudden abdominal, chest or back pain, patients should be advised to immediately consult a physician in an emergency department.
Clostridioides difficile-Associated Diarrhea: Clostridioides difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including AVELOX, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibacterial use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
Arthropathic Effects in Animals: In immature dogs, oral administration of AVELOX caused lameness. Histopathological examination of the weight-bearing joints of these dogs revealed permanent lesions of the cartilage. Related quinolone-class drugs also produce erosions of cartilage of weight-bearing joints and other signs of arthropathy in immature animals of various species (see Pharmacology: Toxicology: Non-clinical Toxicology under Actions).
Blood Glucose Disturbances: As with all fluoroquinolones, disturbances in blood glucose, including both hypoglycemia and hyperglycemia have been reported with AVELOX. In AVELOX-treated patients, dysglycemia occurred predominantly in elderly diabetic patients receiving concomitant treatment with an oral hypoglycemic agent (for example, sulfonylurea) or with insulin. Severe cases of hypoglycemia resulting in coma or death have been reported. In diabetic patients, careful monitoring of blood glucose is recommended. If a hypoglycemic reaction occurs, AVELOX should be discontinued and appropriate therapy should be initiated immediately (see Adverse Reactions and Interactions).
Photosensitivity/Phototoxicity: Moderate to severe photosensitivity/phototoxicity reactions, the latter of which may manifest as exaggerated sunburn reactions (for example, burning, erythema, exudation, vesicles, blistering, edema) involving areas exposed to light (typically the face, "V" area of the neck, extensor surfaces of the forearms, dorsa of the hands), can be associated with the use of fluoroquinolones, including AVELOX, after sun or UV light exposure. Therefore, excessive exposure to these sources of light should be avoided. AVELOX should be discontinued if phototoxicity occurs (see Pharmacology: Pharmacodynamics under Actions).
Development of Drug Resistant Bacteria: Prescribing AVELOX in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Vision disorders: If vision becomes impaired or any effects on the eyes are experienced, an eye specialist should be consulted immediately.
Use in Specific Populations: Renal Impairment: The pharmacokinetic parameters of moxifloxacin are not significantly altered in mild, moderate, severe, or end-stage renal disease. No dosage adjustment is necessary in patients with renal impairment, including those patients requiring hemodialysis (HD) or continuous ambulatory peritoneal dialysis (CAPD) (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions).
Hepatic Impairment: No dosage adjustment is recommended for mild, moderate, or severe hepatic insufficiency (Child-Pugh Classes A, B, or C). However, due to metabolic disturbances associated with hepatic insufficiency, which may lead to QT prolongation, AVELOX should be used with caution in these patients (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Use in Children: Effectiveness in pediatric patients and adolescents less than 18 years of age has not been established. AVELOX causes arthropathy in juvenile animals. Limited information on the safety of AVELOX in 301 pediatric patients is available from the cIAI trial (see Precautions and Pharmacology: Toxicology: Non-clinical Toxicology under Actions).
Active Controlled Trial in Complicated Intra-Abdominal Infection (cIAI): The safety and efficacy of AVELOX in pediatric patients for the treatment of cIAI has not been demonstrated.
Pediatric patients 3 months to <18 years of age (mean age of 12 ± 4 years) were enrolled in a single randomized, double-blind, active controlled trial in cIAI including appendicitis with perforation, abscesses and peritonitis.
Pediatric patients were randomized (2:1) to receive either AVELOX or comparator. This study enrolled 451 patients who received study medication, 301 treated with moxifloxacin, and 150 with comparator. Of the 301 pediatric patients treated with AVELOX, 15 were below the age of 6 years and 286 were between the ages of 6-<18 years.
Patients received sequential intravenous/oral AVELOX or comparator (intravenous ertapenem followed by oral amoxicillin/clavulanate) for 5 to 14 days (mean duration was 9 days with a range of 1 to 24 days).
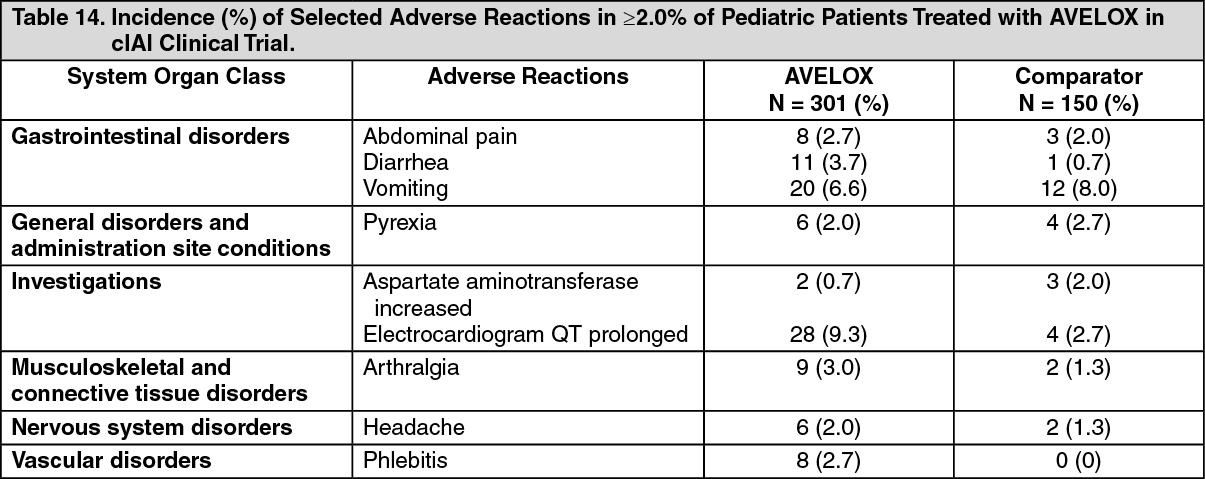
The overall adverse reaction profile in pediatric patients was comparable to that of adult patients. The most frequently occurring adverse reactions in pediatric patients treated with AVELOX were QT prolongation 9.3% (28/301), vomiting, 6.6% (20/301) diarrhea 3.7% (11/301), arthralgia 3.0% (9/301), and phlebitis 2.7% (8/301) (see Table 14). Discontinuation of study drug due to an adverse reaction was reported in 5.3% (16/301) of AVELOX-treated patients versus 1.3% (2/150) of comparator-treated patients. The adverse reaction profile of AVELOX or comparator was similar across all age groups studied.
Musculoskeletal adverse reactions were monitored and followed up to 5 years after the end of study treatment. The rates of musculoskeletal adverse reactions were 4.3% (13/301) in the AVELOX-treated group versus 3.3% (5/150) in the comparator-treated group. The majority of musculoskeletal adverse reactions were reported between 12 and 53 weeks after start of study treatment with complete resolution at the end of the study (see Precautions and Pharmacology: Toxicology: Non-clinical Toxicology under Actions). (See Table 14.)
 Click on icon to see table/diagram/image
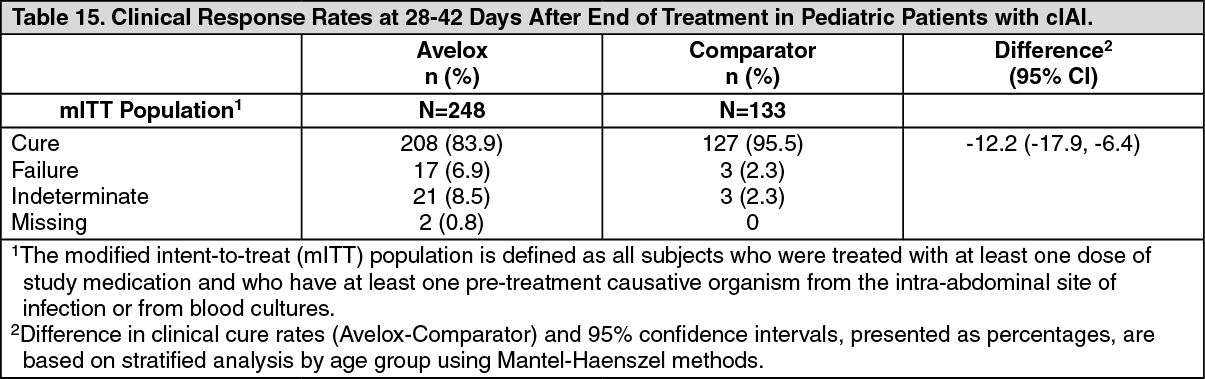
Click on icon to see table/diagram/imageClinical response was assessed at the test-of-cure visit (28 to 42 days after end of treatment). The clinical response rates observed in the modified intent to treat population were 83.9% (208/248) for AVELOX and 95.5% (127/133) for comparator; see Table 15.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUse in the Elderly: Geriatric patients are at increased risk for developing severe tendon disorders including tendon rupture when being treated with a fluoroquinolone such as AVELOX. This risk is further increased in patients receiving concomitant corticosteroid therapy. Tendinitis or tendon rupture can involve the Achilles, hand, shoulder, or other tendon sites and can occur during or after completion of therapy; cases occurring up to several months after fluoroquinolone treatment have been reported. Caution should be used when prescribing AVELOX to elderly patients especially those on corticosteroids. Patients should be informed of this potential side effect and advised to discontinue AVELOX and contact their doctor if any symptoms of tendinitis or tendon rupture occur (see Precautions).
Epidemiologic studies report and increased rate of aortic aneurysm and dissection within two months following use of fluoroquinolones, particularly in elderly patients (see Precautions).
In controlled multiple-dose clinical trials, 23% of patients receiving oral AVELOX were greater than or equal to 65 years of age and 9% were greater than or equal to 75 years of age. The clinical trial data demonstrate that there is no difference in the safety and efficacy of oral AVELOX in patients aged 65 or older compared to younger adults.
In trials of intravenous use, 42% of AVELOX patients were greater than or equal to 65 years of age, and 23% were greater than or equal to 75 years of age. The clinical trial data demonstrate that the safety of intravenous AVELOX in patients aged 65 or older was similar to that of comparator-treated patients. In general, elderly patients may be more susceptible to drug-associated effects of the QT interval. Therefore, AVELOX should be avoided in patients taking drugs that can result in prolongation of the QT interval (for example, class IA or class III antiarrhythmics) or in patients with risk factors for torsade de pointes (for example, known QT prolongation, uncorrected hypokalemia) (see Precautions, Interactions, and Pharmacology: Pharmacokinetics under Actions).