


 Sign Out
Sign Out



In patients with advanced or recurrent solid tumours (N = 515), the most common adverse reactions (>10%) were anaemia (25.6%), nausea (25.0%), diarrhoea (22.5%), vomiting (18.4%), arthralgia (13.8%), pruritus (11.5%), rash (11.1%), pyrexia (10.5%) and hypothyroidism (10.1%). JEMPERLI was permanently discontinued due to adverse reactions in 17 (3.3%) patients; most of them were immune-related events. Adverse reactions were serious in 8.7% of patients; most serious adverse reactions were immune-related adverse reactions (see Precautions).
The safety profile for patients with dMMR/MSI-H endometrial cancer in the GARNET study (N = 129) was not different from that of the overall monotherapy population presented in Table 4.
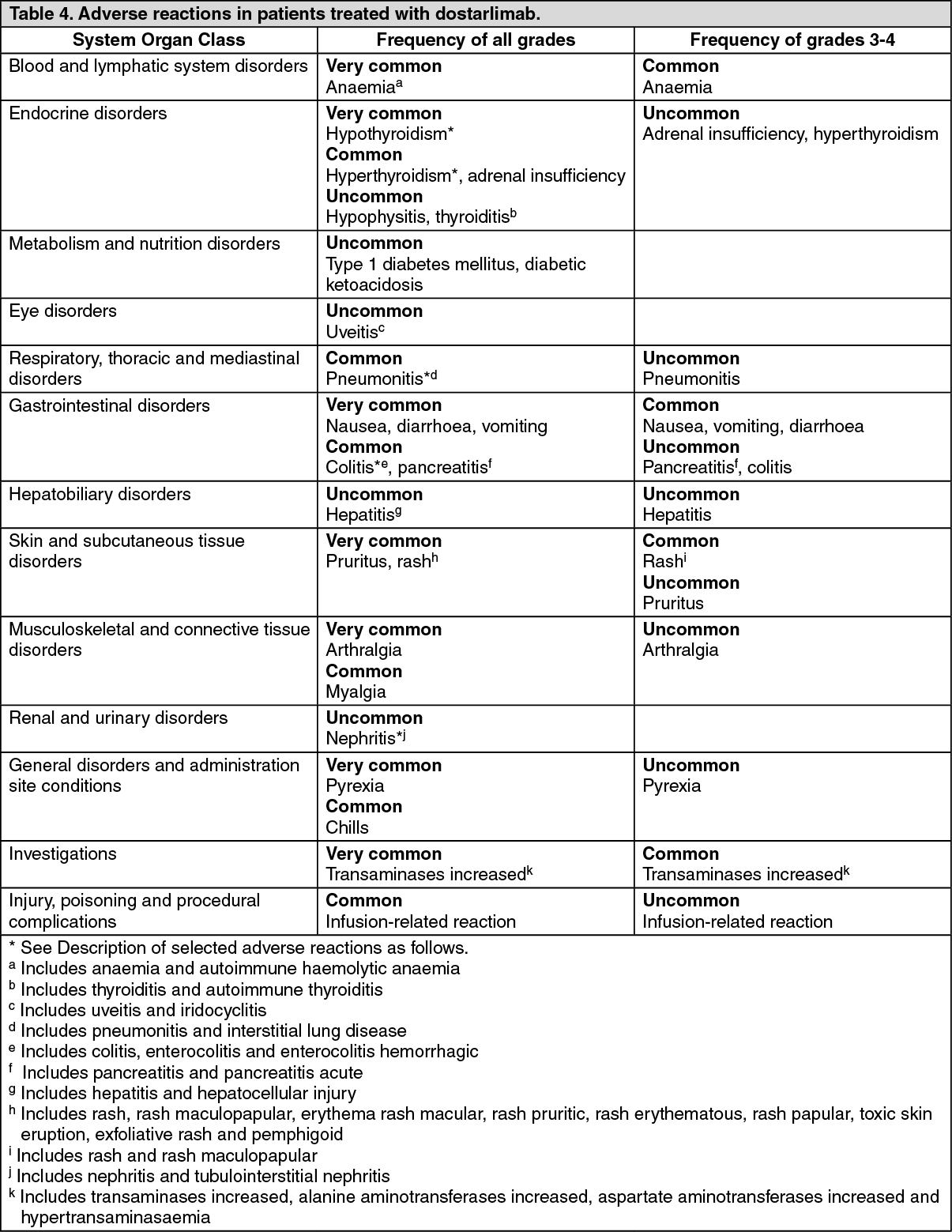
Tabulated list of adverse reactions: Adverse reactions observed in 515 patients with advanced or recurrent solid tumours in the GARNET study of dostarlimab are listed in Table 4. The median duration of treatment in 515 evaluated patients was 20 weeks (range: 1 week to 146 weeks). The frequencies included as follows are based on all reported adverse drug reactions, regardless of the investigator assessment of causality.
These reactions are presented by system organ class and by frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); and not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in the order of decreasing seriousness. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: The selected adverse reactions described as follows are based on the safety of dostarlimab in a combined monotherapy safety database of 515 patients in the GARNET study in patients with endometrial cancer or other advanced solid tumours. Immune-related adverse reactions were defined as events of Grade 2 and above; the following frequencies exclude Grade 1 events. The management guidelines for these adverse reactions are described in Dosage & Administration.
Immune-related adverse reactions (see Precautions): Immune-related pneumonitis: Immune-related pneumonitis occurred in 7 (1.4%) of 515 patients, including Grade 2 (1.2%) and Grade 3 (0.2%) pneumonitis. Pneumonitis led to discontinuation of dostarlimab in 3 (0.6%) patients.
Systemic corticosteroids (prednisone ≥40 mg per day or equivalent) were required in all 7 patients experiencing pneumonitis. Pneumonitis resolved in 6 (85.7%) patients.
Immune-related colitis: Colitis occurred in 8 (1.6%) patients, including Grade 2 (1.0%) and Grade 3 (0.6%) colitis. Colitis did not lead to discontinuation of dostarlimab in any patients.
Systemic corticosteroids (prednisone ≥40 mg per day or equivalent) were required in 2 (28.6%) patients. Colitis resolved in 6 (75.0%) patients experiencing colitis.
Immune-related hepatitis: Hepatitis occurred in 1 (0.2%) patient, which was Grade 3. Systemic corticosteroids (prednisone ≥40 mg per day or equivalent) were required. Hepatitis did not lead to discontinuation of dostarlimab and resolved.
Immune-mediated endocrinopathies: Hypothyroidism occurred in 37 (7.2%) patients, all of which were Grade 2. Hypothyroidism did not lead to discontinuation of dostarlimab and resolved in 13 (35.1%) patients.
Hyperthyroidism occurred in 10 (1.9%) patients, including Grade 2 (1.7%) and Grade 3 (0.2%). Hyperthyroidism did not lead to discontinuation of dostarlimab and resolved in 8 (80%) patients.
Thyroiditis occurred in 2 (0.4%) patients; both were Grade 2. Neither event of thyroiditis resolved; there were no discontinuations of dostarlimab due to thyroiditis.
Adrenal insufficiency occurred in 7 (1.4%) patients, including Grade 2 (0.8%), and Grade 3 (0.6%). Adrenal insufficiency resulted in discontinuation of dostarlimab in 1 (0.2%) patient and resolved in 2 (28.6%) patients.
Immune-mediated nephritis: Nephritis, including tubulointerstitial nephritis, occurred in 3 (0.6%) patients; all were Grade 2. Systemic corticosteroids (prednisone ≥40 mg per day or equivalent) were required in 2 (66.7%) patients experiencing nephritis. Nephritis led to discontinuation of dostarlimab in 1 (0.2%) patient and resolved in 2 of 3 (66.7%) patients.
Immune-related rash: Immune-related rash (rash, rash maculo-papular, rash macular, rash pruritic, pemphigoid) occurred in 17 (3.3%) patients, including Grade 3 in 6 (1.2%) patients receiving dostarlimab. The median time to onset of rash was 41 days (range 2 days to 407 days). Systemic corticosteroids (prednisone ≥40 mg per day or equivalent) were required in 5 (29%) patients experiencing rash. Rash did not lead to discontinuation of dostarlimab and resolved in 13 (76.5%) patients.
Immune-related arthralgia: Immune-related arthralgia occurred in 21 (4.1%) patients. Grade 3 immune-related arthralgia was reported in 3 (0.6%) patients receiving dostarlimab. The median time to onset of arthralgia was 87 days (range 1 day to 783 days). Systemic corticosteroids (prednisone ≥40 mg per day or equivalent) were required in 2 (9.5%) patients experiencing arthralgia. Arthralgia did not lead to discontinuation of dostarlimab and resolved in 8 (38%) patients experiencing arthralgia.
Infusion-related reactions: Infusion-related reactions including hypersensitivity occurred in 7 (1.4%) patients, including Grade 2 (1.2%) and Grade 3 (0.2%) infusion-related reactions. All patients recovered from the infusion-related reaction.
Immunogenicity: Anti-drug antibodies (ADA) were tested in 315 patients who received dostarlimab and the incidence of dostarlimab treatment-emergent ADAs was 2.5%. Neutralising antibodies were detected in 1.3% of patients. In the patients who developed anti-dostarlimab antibodies, there was no evidence of altered efficacy or safety of dostarlimab.
Elderly population: Of the 515 patients treated with dostarlimab monotherapy, 50.7% were under 65 years, 37.9% were 65-75 years, and 11.5% were 75 years or older. No overall differences in safety were reported between elderly (≥65 years) and younger patients (<65 years).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions. If any side effects are experienced, talk to the doctor, pharmacist or nurse. This includes any side effects not listed.
View ADR Monitoring Form