


 Sign Out
Sign Out

 Click on icon to see table/diagram/image
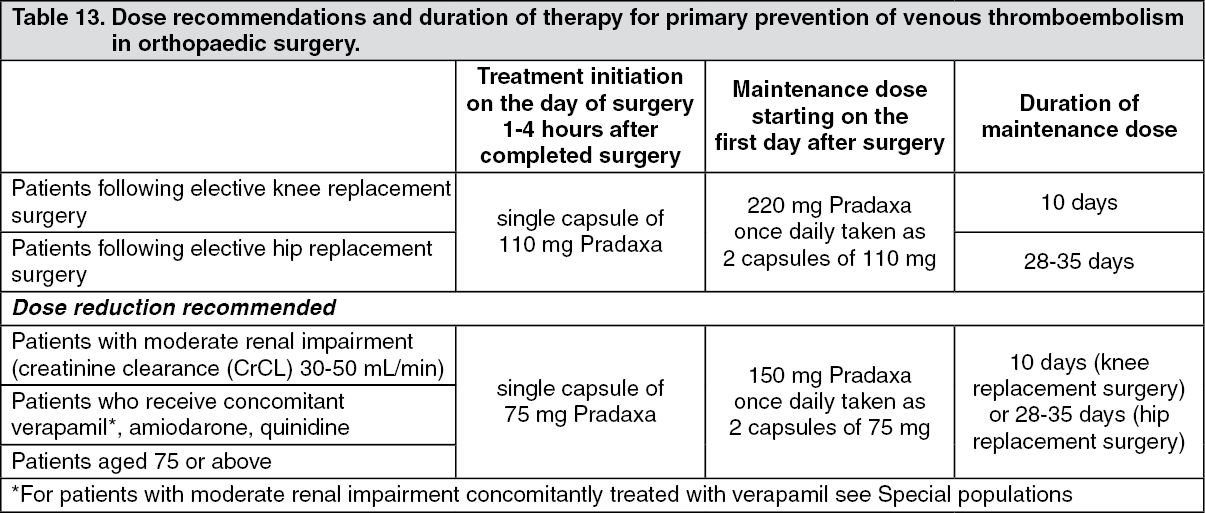
Click on icon to see table/diagram/imageFor both surgeries, if haemostasis is not secured, initiation of treatment should be delayed. If treatment is not started on the day of surgery then treatment should be initiated with 2 capsules once daily.
Assessment of renal function prior to and during Pradaxa treatment: In all patients and especially in the elderly (>75 years), as renal impairment may be frequent in this age group: Renal function should be assessed by calculating the creatinine clearance (CrCL) prior to initiation of treatment with Pradaxa to exclude patients with severe renal impairment (i.e. CrCL < 30 mL/min) (see Contraindications; Precautions; Pharmacology: Pharmacokinetics under Actions).
Renal function should also be assessed when a decline in renal function is suspected during treatment (e.g. hypovolaemia, dehydration, and in case of concomitant use of certain medicinal products).
The method to be used to estimate renal function (CrCL in mL/min) is the Cockcroft-Gault method.
Missed dose: It is recommended to continue with the remaining daily doses of Pradaxa at the same time of the next day.
No double dose should be taken to make up for missed individual doses.
Discontinuation of Pradaxa: Pradaxa treatment should not be discontinued without medical advice. Patients should be instructed to contact the treating physician if they develop gastrointestinal symptoms such as dyspepsia (see Adverse Reactions).
Switching: Pradaxa treatment to parenteral anticoagulant: It is recommended to wait 24 hours after the last dose before switching from Pradaxa to a parenteral anticoagulant (see Interactions).
Parenteral anticoagulants to Pradaxa: The parenteral anticoagulant should be discontinued and Pradaxa should be started 0-2 hours prior to the time that the next dose of the alternate therapy would be due, or at the time of discontinuation in case of continuous treatment (e.g. intravenous Unfractionated Heparin (UFH)) (see Interactions).
Special populations: Renal impairment: Treatment with Pradaxa in patients with severe renal impairment (CrCL < 30 mL/min) is contraindicated (see Contraindications).
In patients with moderate renal impairment (CrCL 30-50 mL/min), a dose reduction is recommended (see Table 13; Precautions; Pharmacology: Pharmacodynamics under Actions).
Concomitant use of Pradaxa with mild to moderate P-glycoprotein (P-gp) inhibitors, i.e. amiodarone, quinidine or verapamil: Dosing should be reduced as indicated in Table 13 (see also Precautions and Interactions). In this situation Pradaxa and these medicinal products should be taken at the same time.
In patients with moderate renal impairment and concomitantly treated with verapamil, a dose reduction of Pradaxa to 75 mg daily should be considered (see Precautions and Interactions).
Elderly: For elderly patients > 75 years, a dose reduction is recommended (see Table 13; Precautions; Pharmacology: Pharmacodynamics under Actions).
Weight: There is very limited clinical experience in patients with a body weight < 50 kg or > 110 kg at the recommended posology. Given the available clinical and kinetic data no adjustment is necessary (see Pharmacology: Pharmacokinetics under Actions), but close clinical surveillance is recommended (see Precautions).
Gender: No dose adjustment is necessary (see Pharmacology: Pharmacokinetics under Actions).
Paediatric population: There is no relevant use of Pradaxa in the paediatric population for the indication of primary prevention of venous thromboembolic events in patients who have undergone elective total hip replacement surgery or total knee replacement surgery.
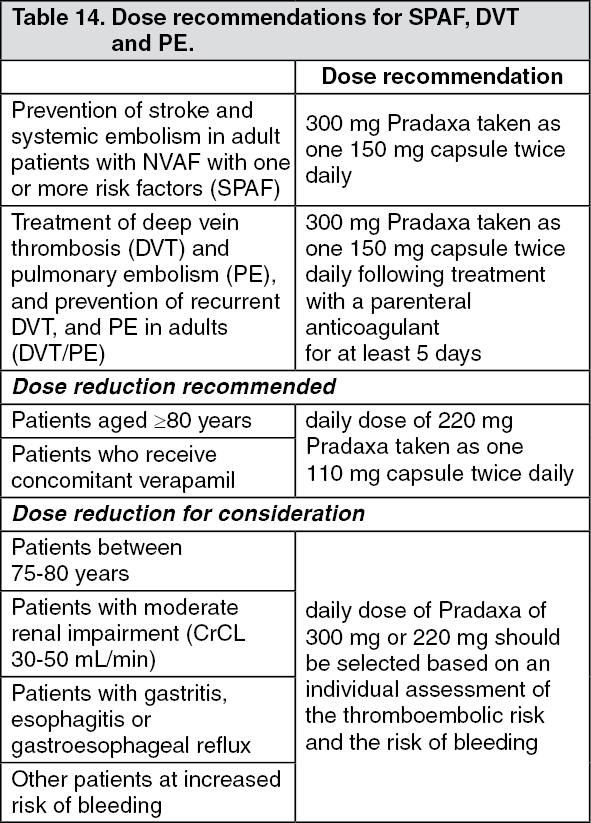
Prevention of stroke and systemic embolism in adult patients with NVAF with one or more risk factors (SPAF): Treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recurrent DVT, and PE in adults (DVT/PE): The recommended doses of Pradaxa in the indications SPAF, DVT and PE are shown in Table 14. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor DVT/PE the recommendation for the use of Pradaxa 220 mg taken as one 110 mg capsule twice daily is based on pharmacokinetic and pharmacodynamic analyses and has not been studied in this clinical setting. See further as follows; Precautions; Interactions; Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions.
In case of intolerability to Pradaxa, patients should be instructed to immediately consult their treating physician in order to be switched to alternate acceptable treatment options for prevention of stroke and systemic embolism associated with atrial fibrillation or for DVT/PE.
Assessment of renal function prior to and during Pradaxa treatment: In all patients and especially in the elderly (>75 years), as renal impairment may be frequent in this age group: Renal function should be assessed by calculating the creatinine clearance (CrCL) prior to initiation of treatment with Pradaxa to exclude patients with severe renal impairment (i.e. CrCL < 30 mL/min) (see Contraindications; Precautions; Pharmacology: Pharmacokinetics under Actions).
Renal function should also be assessed when a decline in renal function is suspected during treatment (e.g. hypovolaemia, dehydration, and in case of concomitant use of certain medicinal products).
Additional requirements in patients with mild to moderate renal impairment and in patients aged over 75 years: Renal function should be assessed during treatment with Pradaxa at least once a year or more frequently as needed in certain clinical situations when it is suspected that the renal function could decline or deteriorate (e.g. hypovolaemia, dehydration, and in case of concomitant use of certain medicinal products).
The method to be used to estimate renal function (CrCL in mL/min) is the Cockcroft-Gault method.
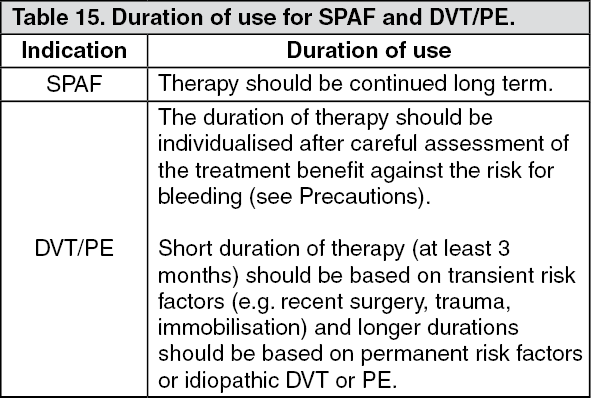
Duration of use: The duration of use of Pradaxa in the indications SPAF, DVT and PE are shown in Table 15. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMissed dose: A forgotten Pradaxa dose may still be taken up to 6 hours prior to the next scheduled dose. From 6 hours prior to the next scheduled dose on, the missed dose should be omitted.
No double dose should be taken to make up for missed individual doses.
Discontinuation of Pradaxa: Pradaxa treatment should not be discontinued without medical advice. Patients should be instructed to contact the treating physician if they develop gastrointestinal symptoms such as dyspepsia (see Adverse Reactions).
Switching: Pradaxa treatment to parenteral anticoagulant: It is recommended to wait 12 hours after the last dose before switching from Pradaxa to a parenteral anticoagulant (see Interactions).
Parenteral anticoagulants to Pradaxa: The parenteral anticoagulant should be discontinued and Pradaxa should be started 0-2 hours prior to the time that the next dose of the alternate therapy would be due, or at the time of discontinuation in case of continuous treatment (e.g. intravenous Unfractionated Heparin (UFH)) (see Interactions).
Pradaxa treatment to Vitamin K antagonists (VKA): The starting time of the VKA should be adjusted based on CrCL as follows: CrCL ≥ 50 mL/min, VKA should be started 3 days before discontinuing Pradaxa; CrCL ≥ 30-< 50 mL/min, VKA should be started 2 days before discontinuing Pradaxa.
Because Pradaxa can impact the International Normalized Ratio (INR), the INR will better reflect VKA's effect only after Pradaxa has been stopped for at least 2 days. Until then, INR values should be interpreted with caution.
VKA to Pradaxa: The VKA should be stopped. Pradaxa can be given as soon as the INR is < 2.0.
Cardioversion (SPAF): Patients can stay on Pradaxa while being cardioverted.
Catheter ablation for atrial fibrillation (SPAF): There are no data available for 110 mg twice daily Pradaxa treatment.
Catheter ablation can be conducted in patients on 150 mg twice daily Pradaxa treatment. Pradaxa treatment does not need to be interrupted (see Pharmacology: Pharmacodynamics under Actions).
Percutaneous coronary intervention (PCI) with stenting (SPAF): Patients with non valvular atrial fibrillation who undergo a PCI with stenting can be treated with Pradaxa in combination with antiplatelets after haemostasis is achieved (see Pharmacology: Pharmacodynamics under Actions).
Special populations: Elderly: For dose modifications in this population see Table 14.
Patients at risk of bleeding: Patients with an increased bleeding risk (see Precautions; Interactions; Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions) should be closely monitored clinically (looking for signs of bleeding or anaemia). Dose adjustment should be decided at the discretion of the physician, following assessment of the potential benefit and risk to an individual patient (see Table 14). A coagulation test (see Precautions) may help to identify patients with an increased bleeding risk caused by excessive dabigatran exposure. When excessive dabigatran exposure is identified in patients at high risk of bleeding, a reduced dose of 220 mg taken as one 110 mg capsule twice daily is recommended. When clinically relevant bleeding occurs, treatment should be interrupted.
For subjects with gastritis, esophagitis, or gastroesophageal reflux, a dose reduction may be considered due to the elevated risk of major gastro-intestinal bleeding (see Table 14 and Precautions).
Renal impairment: Treatment with Pradaxa in patients with severe renal impairment (CrCL < 30 mL/min) is contraindicated (see Contraindications).
No dose adjustment is necessary in patients with mild renal impairment (CrCL 50 - ≤ 80 mL/min). For patients with moderate renal impairment (CrCL 30-50 mL/min) the recommended dose of Pradaxa is also 300 mg taken as one 150 mg capsule twice daily. However, for patients with high risk of bleeding, a dose reduction of Pradaxa to 220 mg taken as one 110 mg capsule twice daily should be considered (see Precautions; Pharmacology: Pharmacokinetics under Actions). Close clinical surveillance is recommended in patients with renal impairment.
Concomitant use of Pradaxa with mild to moderate P-glycoprotein (P-gp) inhibitors, i.e. amiodarone, quinidine or verapamil: No dose adjustment is necessary for concomitant use of amiodarone or quinidine (see Precautions; Interactions; Pharmacology: Pharmacokinetics under Actions).
Dose reductions are recommended for patients who receive concomitantly verapamil (see Table 14 and Precautions and Interactions). In this situation Pradaxa and verapamil should be taken at the same time.
Weight: No dose adjustment is necessary (see Pharmacology: Pharmacokinetics under Actions), but close clinical surveillance is recommended in patients with a body weight < 50 kg (see Precautions).
Gender: No dose adjustment is necessary (see Pharmacology: Pharmacokinetics under Actions).
Paediatric population: There is no relevant use of Pradaxa in the paediatric population for the indication of prevention of stroke and systemic embolism in patients with NVAF.
For the indication DVT/PE, the safety and efficacy of Pradaxa in children from birth to less than 18 years of age have not yet been established. Currently available data are described in Adverse Reactions and Pharmacology: Pharmacodynamics under Actions, but no recommendation on a posology can be made.
Method of administration: Pradaxa is for oral use.
The capsules can be taken with or without food. Pradaxa should be swallowed as a whole with a glass of water, to facilitate delivery to the stomach.
Patients should be instructed not to open the capsule as this may increase the risk of bleeding (see Pharmacology: Pharmacokinetics under Actions; Special precautions for other handling under Cautions for Usage).