Pharmacotherapeutic group: antithrombotic agents, direct thrombin inhibitors.
ATC code: B01AE07.
Pharmacology: Pharmacodynamics: Mechanism of action: Dabigatran etexilate is a small molecule prodrug which does not exhibit any pharmacological activity. After oral administration, dabigatran etexilate is rapidly absorbed and converted to dabigatran by esterase-catalysed hydrolysis in plasma and in the liver. Dabigatran is a potent, competitive, reversible direct thrombin inhibitor and is the main active principle in plasma.
Since thrombin (serine protease) enables the conversion of fibrinogen into fibrin during the coagulation cascade, its inhibition prevents the development of thrombus. Dabigatran inhibits free thrombin, fibrin-bound thrombin and thrombin-induced platelet aggregation.
Pharmacodynamic effects: In vivo and
ex vivo animal studies have demonstrated antithrombotic efficacy and anticoagulant activity of dabigatran after intravenous administration and of dabigatran etexilate after oral administration in various animal models of thrombosis.
There is a clear correlation between plasma dabigatran concentration and degree of anticoagulant effect based on phase II studies. Dabigatran prolongs the thrombin time (TT), ECT, and aPTT.
The calibrated quantitative diluted TT (dTT) test provides an estimation of dabigatran plasma concentration that can be compared to the expected dabigatran plasma concentrations. When the calibrated dTT assay delivers a dabigatran plasma concentration result at or below the limit of quantification, an additional coagulation assay such as TT, ECT or aPTT should be considered.
The ECT can provide a direct measure of the activity of direct thrombin inhibitors.
The aPTT test is widely available and provides an approximate indication of the anticoagulation intensity achieved with dabigatran. However, the aPTT test has limited sensitivity and is not suitable for precise quantification of anticoagulant effect, especially at high plasma concentrations of dabigatran. Although high aPTT values should be interpreted with caution, a high aPTT value indicates that the patient is anticoagulated.
In general, it can be assumed that these measures of anti-coagulant activity may reflect dabigatran levels and can provide guidance for the assessment of bleeding risk, i.e. exceeding the 90
th percentile of dabigatran trough levels or a coagulation assay such as aPTT measured at trough (for aPTT thresholds see Precautions, Table 17) is considered to be associated with an increased risk of bleeding.
Primary Prevention of Venous Thromboembolism in Orthopaedic Surgery: Steady state (after day 3) geometric mean dabigatran peak plasma concentration, measured around 2 hours after 220 mg dabigatran etexilate administration, was 70.8 ng/mL, with a range of 35.2-162 ng/mL (25
th-75
th percentile range). The dabigatran geometric mean trough concentration, measured at the end of the dosing interval (i.e. 24 hours after a 220 mg dabigatran dose), was on average 22.0 ng/mL, with a range of 13.0-35.7 ng/mL (25
th-75
th percentile range).
In a dedicated study exclusively in patients with moderate renal impairment (creatinine clearance, CrCL 30-50 mL/min) treated with dabigatran etexilate 150 mg QD, the dabigatran geometric mean trough concentration, measured at the end of the dosing interval, was on average 47.5 ng/mL, with a range of 29.6 - 72.2 ng/mL (25
th-75
th percentile range).
In patients treated for prevention of VTEs after hip or knee replacement surgery with 220 mg dabigatran etexilate once daily: the 90
th percentile of dabigatran plasma concentrations was 67 ng/mL, measured at trough (20-28 hours after the previous dose) (see Precautions and Overdosage); the 90
th percentile of aPTT at trough (20-28 hours after the previous dose) was 51 seconds, which would be 1.3-fold upper limit of normal.
The ECT was not measured in patients treated for prevention of VTEs after hip or knee replacement surgery with 220 mg dabigatran etexilate once daily.
Prevention of stroke and systemic embolism in adult patients with NVAF with one or more risk factors (SPAF): Steady state geometric mean dabigatran peak plasma concentration, measured around 2 hours after 150 mg dabigatran etexilate administration twice daily, was 175 ng/mL, with a range of 117-275 ng/mL (25
th-75
th percentile range). The dabigatran geometric mean trough concentration, measured at trough in the morning, at the end of the dosing interval (i.e. 12 hours after the 150 mg dabigatran evening dose), was on average 91.0 ng/mL, with a range of 61.0-143 ng/mL (25
th-75
th percentile range).
For patients with NVAF treated for prevention of stroke and systemic embolism with 150 mg dabigatran etexilate twice daily: the 90
th percentile of dabigatran plasma concentrations measured at trough (10-16 hours after the previous dose) was about 200 ng/mL; an ECT at trough (10-16 hours after the previous dose), elevated approximately 3-fold upper limit of normal refers to the observed 90
th percentile of ECT prolongation of 103 seconds; an aPTT ratio greater than 2-fold upper limit of normal (aPTT prolongation of about 80 seconds), at trough (10-16 hours after the previous dose) reflects the 90
th percentile of observations.
Treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recurrent DVT and PE in adults (DVT/PE): In patients treated for DVT and PE with 150 mg dabigatran etexilate twice daily, the dabigatran geometric mean trough concentration, measured within 10-16 hours after dose, at the end of the dosing interval (i.e. 12 hours after the 150 mg dabigatran evening dose), was 59.7 ng/mL, with a range of 38.6 - 94.5 ng/mL (25
th-75
th percentile range). For treatment of DVT and PE, with dabigatran etexilate 150 mg twice daily: the 90
th percentile of dabigatran plasma concentrations measured at trough (10-16 hours after the previous dose) was about 146 ng/mL; an ECT at trough (10-16 hours after the previous dose), elevated approximately 2.3-fold compared to baseline refers to the observed 90
th percentile of ECT prolongation of 74 seconds; the 90
th percentile of aPTT at trough (10-16 hours after the previous dose) was 62 seconds, which would be 1.8-fold compared to baseline.
In patients treated for prevention of recurrent of DVT and PE with 150 mg dabigatran etexilate twice daily no pharmacokinetic data are available.
Clinical efficacy and safety: Ethnic origin: No clinically relevant ethnic differences among Caucasians, African-American, Hispanic, Japanese or Chinese patients were observed.
Clinical trials in Venous Thromboembolism (VTE) prophylaxis following major joint replacement surgery: In 2 large randomized, parallel group, double-blind, dose-confirmatory trials, patients undergoing elective major orthopaedic surgery (one for knee replacement surgery and one for hip replacement surgery) received Pradaxa 75 mg or 110 mg within 1-4 hours of surgery followed by 150 mg or 220 mg once daily thereafter, haemostasis having been secured, or enoxaparin 40 mg on the day prior to surgery and daily thereafter.
In the RE-MODEL trial (knee replacement) treatment was for 6-10 days and in the RE-NOVATE trial (hip replacement) for 28-35 days. Totals of 2,076 patients (knee) and 3,494 (hip) were treated respectively.
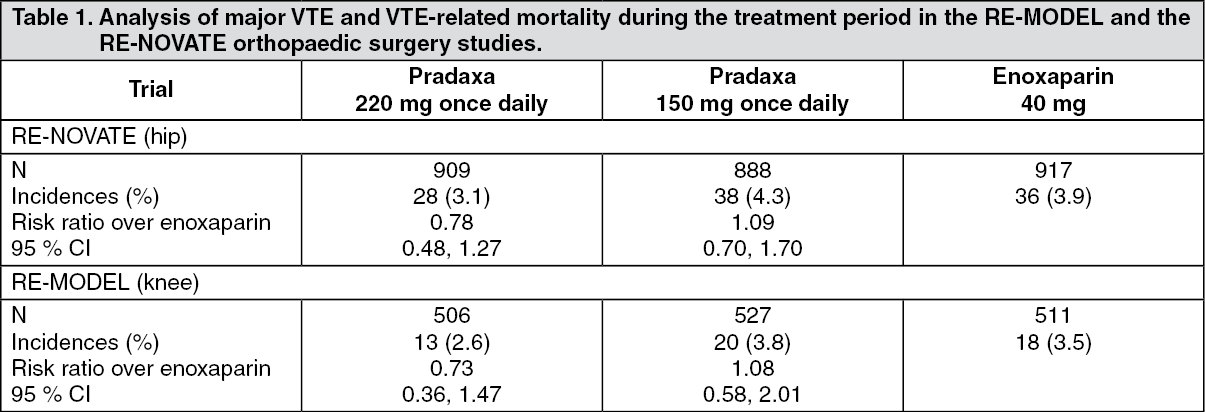
Composite of total VTE (including PE, proximal and distal DVT, whatever symptomatic or asymptomatic detected by routine venography) and all-cause mortality constituted the primary end-point for both studies. Composite of major VTE (including PE and proximal DVT, whatever symptomatic or asymptomatic detected by routine venography) and VTE-related mortality constituted a secondary end-point and is considered of better clinical relevance.
Results of both studies showed that the antithrombotic effect of Pradaxa 220 mg and 150 mg were statistically non-inferior to that of enoxaparin on total VTE and all-cause mortality. The point estimate for incidence of Major VTE and VTE related mortality for the 150 mg dose was slightly worse than enoxaparin (Table 1). Better results were seen with the 220 mg dose where the point estimate of Major VTE was slightly better than enoxaparin (Table 1).
The clinical studies have been conducted in a patient population with a mean age > 65 years.
There were no differences in the phase 3 clinical studies for efficacy and safety data between men and women.
In the studied patient population of RE-MODEL and RE-NOVATE (5,539 patients treated), 51 % suffered from concomitant hypertension, 9 % from concomitant diabetes, 9 % from concomitant coronary artery disease and 20 % had a history of venous insufficiency. None of these diseases showed an impact on the effects of dabigatran on VTE-prevention or bleeding rates.
Data for the major VTE and VTE-related mortality endpoint were homogeneous with regards to the primary efficacy endpoint and are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Data for the total VTE and all cause mortality endpoint are shown in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
Data for adjudicated major bleeding endpoints are shown in Table 3 as follows. (See Table 3.)
Click on icon to see table/diagram/image
Prevention of stroke and systemic embolism in adult patients with NVAF with one or more risk factors: The clinical evidence for the efficacy of dabigatran etexilate is derived from the RE-LY study (Randomized Evaluation of Long-term anticoagulant therapy) a multi-centre, multi-national, randomized parallel group study of two blinded doses of dabigatran etexilate (110 mg and 150 mg twice daily) compared to open-label warfarin in patients with atrial fibrillation at moderate to high risk of stroke and systemic embolism. The primary objective in this study was to determine if dabigatran etexilate was non-inferior to warfarin in reducing the occurrence of the composite endpoint stroke and systemic embolism. Statistical superiority was also analysed.
In the RE-LY study, a total of 18,113 patients were randomized, with a mean age of 71.5 years and a mean CHADS
2 score of 2.1. The patient population was 64 % male, 70 % Caucasian and 16 % Asian. For patients randomized to warfarin, the mean percentage of time in therapeutic range (TTR) (INR 2-3) was 64.4 % (median TTR 67 %).
The RE-LY study demonstrated that dabigatran etexilate, at a dose of 110 mg twice daily, is non-inferior to warfarin in the prevention of stroke and systemic embolism in subjects with atrial fibrillation, with a reduced risk of ICH, total bleeding and major bleeding. The dose of 150 mg twice daily reduces significantly the risk of ischemic and haemorrhagic stroke, vascular death, ICH and total bleeding compared to warfarin. Major bleeding rates with this dose were comparable to warfarin. Myocardial infarction rates were slightly increased with dabigatran etexilate 110 mg twice daily and 150 mg twice daily compared to warfarin (hazard ratio 1.29; p=0.0929 and hazard ratio 1.27; p=0.1240, respectively). With improving monitoring of INR the observed benefits of dabigatran etexilate compared to warfarin diminish.
Tables 4-6 display details of key results in the overall population: See Tables 4, 5 and 6.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Tables 7-9 display results of the primary efficacy and safety endpoint in relevant sub-populations: For the primary endpoint, stroke and systemic embolism, no subgroups (i.e., age, weight, gender, renal function, ethnicity, etc.) were identified with a different risk ratio compared to warfarin. (See Table 7.)
Click on icon to see table/diagram/image
For the primary safety endpoint of major bleeding there was an interaction of treatment effect and age. The relative risk of bleeding with dabigatran compared to warfarin increased with age. Relative risk was highest in patients ≥ 75 years. The concomitant use of antiplatelets ASA or clopidogrel approximately doubles MBE rates with both dabigatran etexilate and warfarin. There was no significant interaction of treatment effects with the subgroups of renal function and CHADS
2 score. (See Table 8.)
Click on icon to see table/diagram/image
RELY-ABLE (Long term multi-center extension of dabigatran treatment in patients with atrial fibrillation who completed the RE-LY trial): The RE-LY extension study (RELY-ABLE) provided additional safety information for a cohort of patients which continued the same dose of dabigatran etexilate as assigned in the RE-LY trial. Patients were eligible for the RELY-ABLE trial if they had not permanently discontinued study medication at the time of their final RE-LY study visit. Enrolled patients continued to receive the same double-blind dabigatran etexilate dose randomly allocated in RE-LY, for up to 43 months of follow up after RE-LY (total mean follow-up RE-LY + RELY-ABLE, 4.5 years). There were 5897 patients enrolled, representing 49 % of patients originally randomly assigned to receive dabigatran etexilate in RE-LY and 86 % of RELY-ABLE-eligible patients.
During the additional 2.5 years of treatment in RELY-ABLE, with a maximum exposure of over 6 years (total exposure in RELY + RELY-ABLE), the long-term safety profile of dabigatran etexilate was confirmed for both test doses 110 mg b.i.d. and 150 mg b.i.d.. No new safety findings were observed.
The rates of outcome events including, major bleed and other bleeding events were consistent with those seen in RE-LY.
Data from non-interventional studies: A non-interventional study (GLORIA-AF) prospectively collected (in its second phase) safety and effectiveness data in newly diagnosed NVAF patients on dabigatran etexilate in a real-world setting. The study included 4,859 patients on dabigatran etexilate (55% treated with 150 mg bid, 43% treated with 110 mg bid, 2% treated with 75 mg bid). Patients were followed-up for 2 years. The mean CHADS
2 and HAS-BLED scores were 1.9 and 1.2, respectively. Mean on-therapy follow-up time was 18.3 months. Major bleeding occurred in 0.97 per 100 patient-years. Life-threatening bleeding was reported in 0.46 per 100 patient-years, intracranial haemorrhage in 0.17 per 100 patient-years and gastrointestinal bleeding in 0.60 per 100 patient-years. Stroke occurred in 0.65 per 100 patient-years.
In addition, in a non-interventional study [Graham DJ et al., Circulation. 2015;131:157-164] in more than 134,000 elderly patients with NVAF in the United States (contributing more than 37,500 patient-years of on-therapy follow-up time) dabigatran etexilate (84 % patients treated with 150 mg bid, 16 % patients treated with 75 mg bid) was associated with a reduced risk of ischemic stroke (hazard ratio 0.80, 95 % confidence interval [CI] 0.67 - 0.96), intracranial haemorrhage (hazard ratio 0.34, CI 0.26 - 0.46), and mortality (hazard ratio 0.86, CI 0.77 - 0.96) and increased risk of gastrointestinal bleeding (hazard ratio 1.28, CI 1.14 - 1.44) compared to warfarin. No difference was found for major bleeding (hazard ratio 0.97, CI 0.88 - 1.07).
These observations in real-world settings are consistent with the established safety and efficacy profile for dabigatran etexilate in the RE-LY study in this indication.
Patients undergoing catheter ablation for atrial fibrillation: A prospective, randomized, open-label, multicenter, exploratory study with blinded, centrally adjudicated endpoint evaluation (RE-CIRCUIT) was conducted in 704 patients who were under stable anticoagulant treatment. The study compared 150 mg twice daily uninterrupted dabigatran etexilate with uninterrupted INR-adjusted warfarin in catheter ablation of paroxysmal or persistent atrial fibrillation. Of the 704 enrolled patients, 317 underwent atrial fibrillation ablation on uninterrupted dabigatran and 318 underwent atrial fibrillation ablation on uninterrupted warfarin. All patients underwent a Trans-oesophageal Echocardiography (TEE) prior to catheter ablation. The primary outcome (adjudicated major bleeding according to ISTH criteria) occurred in 5 (1.6 %) patients in the dabigatran etexilate group and 22 (6.9 %) patients in the warfarin group (risk difference -5.3%; 95% CI -8.4, -2.2; P=0.0009). There was no stroke/systemic embolism/TIA (composite) event in the dabigatran etexilate arm, and one event (TIA) in the warfarin arm from the time of ablation and until 8 weeks post-ablation. This exploratory study showed that dabigatran etexilate was associated with a significant reduction in MBE rate compared with INR-adjusted warfarin in the setting of ablation.
Patients who underwent Percutaneous coronary intervention (PCI) with stenting: A prospective, randomized, open-label, blinded endpoint (PROBE) study (Phase IIIb) to evaluate dual-therapy with dabigatran etexilate (110 mg or 150 mg bid) plus clopidogrel or ticagrelor (P2Y12 antagonist) vs. triple-therapy with warfarin (adjusted to a INR 2.0 - 3.0) plus clopidogrel or ticagrelor and aspirin was conducted in 2725 patients with non valvular atrial fibrillation who underwent a PCI with stenting (RE-DUAL PCI). Patients were randomized to dabigatran etexilate 110 mg bid dual-therapy, dabigatran etexilate 150 mg bid dual-therapy or warfarin triple-therapy. Elderly patients outside of the United States (≥80 years of age for all countries, ≥70 years of age for Japan) were randomly assigned to the dabigatran etexilate 110 mg dual-therapy group or the warfarin triple-therapy group. The primary endpoint was a combined endpoint of major bleeds based on ISTH definition or clinically relevant non-major bleeding event.
The incidence of the primary endpoint was 15.4 % (151 patients) in the dabigatran etexilate 110 mg dual-therapy group as compared with 26.9 % (264 patients) in the warfarin triple-therapy group (HR 0.52; 95% CI 0.42, 0.63; P<0.0001 for non-inferiority and P<0.0001 for superiority) and 20.2 % (154 patients) in the dabigatran etexilate 150 mg dual-therapy group as compared with 25.7 % (196 patients) in the corresponding warfarin triple-therapy group (HR 0.72; 95% CI 0.58, 0.88; P<0.0001 for non-inferiority and P=0.002 for superiority). As part of the descriptive analysis, TIMI (Thrombolysis In Myocardial Infarction) major bleeding events was lower in both dabigatran etexilate dual-therapy groups than in the warfarin triple-therapy group: 14 events (1.4%) in the dabigatran etexilate 110 mg dual-therapy group as compared with 37 events (3.8%) in the warfarin triple-therapy group (HR 0.37; 95% CI 0.20, 0.68; P=0.002) and 16 events (2.1%) in the dabigatran etexilate 150 mg dual-therapy group as compared with 30 events (3.9%) in the corresponding warfarin triple-therapy group (HR 0.51; 95% CI 0.28, 0.93; P=0.03). Both dabigatran etexilate dual-therapy groups had lower rates of intracranial hemorrhage than the corresponding warfarin triple-therapy group: 3 events (0.3%) in the 110 mg dabigatran etexilate dual-therapy group as compared with 10 events (1.0%) in the warfarin triple-therapy group (HR 0.30; 95% CI 0.08, 1.07; P=0.06) and 1 event (0.1%) in the 150 mg dabigatran etexilate dual-therapy group as compared with 8 events (1.0%) in the corresponding warfarin triple-therapy group (HR 0.12; 95% CI 0.02, 0.98; P=0.047). The incidence of the composite efficacy endpoint of death, thromboembolic events (myocardial infarction, stroke, or systemic embolism) or unplanned revascularization in the two dabigatran etexilate dual-therapy groups combined was non-inferior to the warfarin triple-therapy group (13.7% vs. 13.4% respectively; HR 1.04; 95% CI: 0.84, 1.29; P=0.0047 for non-inferiority). There were no statistical differences in the individual components of the efficacy endpoints between either dabigatran etexilate dual-therapy groups and warfarin triple-therapy.
This study demonstrated that dual-therapy, with dabigatran etexilate and a P2Y12 antagonist, significantly reduced the risk of bleeding vs. warfarin triple-therapy, with non-inferiority for composite of thromboembolic events, in patients with atrial fibrillation who underwent a PCI with stenting.
Treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) in adults (DVT/PE treatment): The efficacy and safety was investigated in two multi-center, randomised, double blind, parallel-group, replicate studies RE-COVER and RE-COVER II. These studies compared dabigatran etexilate (150 mg bid) with warfarin (target INR 2.0-3.0) in patients with acute DVT and/or PE. The primary objective of these studies was to determine if dabigatran etexilate was non-inferior to warfarin in reducing the occurrence of the primary endpoint which was the composite of recurrent symptomatic DVT and/or PE and related deaths within the 6 month treatment period.
In the pooled RE-COVER and RE-COVER II studies, a total of 5,153 patients were randomised and 5,107 were treated.
The duration of treatment with fixed dose of dabigatran was 174.0 days without coagulation monitoring. For patients randomized to warfarin, the median time in therapeutic range (INR 2.0 to 3.0) was 60.6 %.
The trials, demonstrated that treatment with dabigatran etexilate 150 mg twice daily was non-inferior to the treatment with warfarin (non-inferiority margin for RE-COVER, and RE-COVER II: 3.6 for risk difference and 2.75 for hazard ratio). (See Table 9.)
Click on icon to see table/diagram/image
Prevention of recurrent deep vein thrombosis (DVT) and pulmonary embolism (PE) in adults (DVT/PE prevention): Two randomized, parallel group, double-blind studies were performed in patients previously treated with anticoagulation therapy. RE-MEDY, warfarin controlled study, enrolled patients already treated for 3 to 12 months with the need for further anticoagulant treatment and RE-SONATE, the placebo controlled study, enrolled patients already treated for 6 to 18 months with Vitamin K inhibitors.
The objective of the RE-MEDY study was to compare the safety and efficacy of oral dabigatran etexilate (150 mg bid) to warfarin (target INR 2.0-3.0) for the long-term treatment and prevention of recurrent, symptomatic DVT and/or PE. A total of 2,866 patients were randomized and 2,856 patients were treated. Duration of dabigatran etexilate treatment ranged from 6 to 36 months (median 534.0 days). For patients randomized to warfarin, the median time in therapeutic range (INR 2.0-3.0) was 64.9 %.
RE-MEDY demonstrated that treatment with dabigatran etexilate 150 mg twice daily was non-inferior to warfarin (non-inferiority margin: 2.85 for hazard ratio and 2.8 for risk difference). (See Table 10.)
Click on icon to see table/diagram/image
The objective of the RE-SONATE study was to evaluate superiority of dabigatran etexilate versus placebo for the prevention of recurrent symptomatic DVT and/or PE in patients who had already completed 6 to 18 months of treatment with VKA. The intended therapy was 6 months dabigatran etexilate 150 mg twice daily without need for monitoring.
RE-SONATE demonstrated dabigatran etexilate was superior to placebo for the prevention of recurrent symptomatic DVT/PE events including unexplained deaths, with a risk reduction from 5.6 % to 0.4 % (relative risk reduction 92 % based on hazard ratio) during the treatment period (p<0.0001). All secondary and sensitivity analyses of the primary endpoint and all secondary endpoints showed superiority of dabigatran etexilate over placebo.
The study included observational follow-up for 12 months after the conclusion of treatment. After discontinuation of study medication the effect was maintained until the end of the follow-up, indicating that the initial treatment effect of dabigatran etexilate was sustained. No rebound effect was observed. At the end of the follow-up VTE events in patients treated with dabigatran etexilate was 6.9 % vs. 10.7 % among the placebo group (hazard ratio 0.61 (95% CI 0.42, 0.88), p=0.0082). (See Table 11.)
Click on icon to see table/diagram/image
Clinical trials for the prevention of thromboembolism in patients with prosthetic heart valves: A phase II study examined dabigatran etexilate and warfarin in a total of 252 patients with recent mechanical valve replacement surgery (i.e. within the current hospital stay) and in patients who received a mechanical heart valve replacement more than three months ago. More thromboembolic events (mainly strokes and symptomatic/asymptomatic prosthetic valve thrombosis) and more bleeding events were observed with dabigatran etexilate than with warfarin. In the early post-operative patients, major bleeding manifested predominantly as haemorrhagic pericardial effusions, specifically in patients who started dabigatran etexilate early (i.e. on Day 3) after heart valve replacement surgery (see Contraindications).
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Pradaxa in all subsets of the paediatric population for the granted indications (see Dosage & Administration for information on paediatric use).
The pharmacokinetics and pharmacodynamics of dabigatran etexilate administered twice daily for three consecutive days (total 6 doses) at the end of standard anticoagulant therapy were assessed in an open-label safety and tolerability study in 9 stable adolescents (12 to < 18 years). All patients received an initial oral dose of 1.71 (± 10%) mg/kg of dabigatran etexilate (80 % of the adult dose of 150 mg/70 kg adjusted for the patient's weight). Based on dabigatran concentrations and clinical assessment, the dose was subsequently modified to a target dose of 2.14 (± 10 %) mg/kg of dabigatran etexilate (100 % of the adult dose adjusted for the patient's weight). In this small number of adolescents, dabigatran etexilate capsules were apparently tolerated with only three mild and transient gastrointestinal adverse events reported by two patients. According to the relatively low exposure, coagulation at 72 hrs (presumed dabigatran trough level at steady state or close to steady state conditions) was only slightly prolonged with aPTT at maximum 1.60 fold, ECT 1.86 fold, and Hemoclot TT (Anti-FIIa) 1.36 fold, respectively. Dabigatran plasma concentrations observed at 72 hrs were relatively low, between 32.9 ng/mL and 97.2 ng/mL at final doses between 100 mg and 150 mg (gMean dose normalized total dabigatran plasma concentration of 0.493 ng/mL/mg).
Pharmacokinetics: After oral administration, dabigatran etexilate is rapidly and completely converted to dabigatran, which is the active form in plasma. The cleavage of the prodrug dabigatran etexilate by esterase-catalysed hydrolysis to the active principle dabigatran is the predominant metabolic reaction. The absolute bioavailability of dabigatran following oral administration of Pradaxa was approximately 6.5 %.
After oral administration of Pradaxa in healthy volunteers, the pharmacokinetic profile of dabigatran in plasma is characterized by a rapid increase in plasma concentrations with C
max attained within 0.5 and 2.0 hours post administration.
Absorption: A study evaluating post-operative absorption of dabigatran etexilate, 1-3 hours following surgery, demonstrated relatively slow absorption compared with that in healthy volunteers, showing a smooth plasma concentration-time profile without high peak plasma concentrations. Peak plasma concentrations are reached at 6 hours following administration in a postoperative period due to contributing factors such as anaesthesia, GI paresis, and surgical effects independent of the oral medicinal product formulation. It was demonstrated in a further study that slow and delayed absorption is usually only present on the day of surgery. On subsequent days absorption of dabigatran is rapid with peak plasma concentrations attained 2 hours after medicinal product administration.
Food does not affect the bioavailability of dabigatran etexilate but delays the time to peak plasma concentrations by 2 hours.
C
max and AUC were dose proportional.
The oral bioavailability may be increased by 75 % after a single dose and 37 % at steady state compared to the reference capsule formulation when the pellets are taken without the Hydroxypropylmethylcellulose (HPMC) capsule shell. Hence, the integrity of the HPMC capsules should always be preserved in clinical use to avoid unintentionally increased bioavailability of dabigatran etexilate (see Dosage & Administration).
Distribution: Low (34-35 %) concentration independent binding of dabigatran to human plasma proteins was observed. The volume of distribution of dabigatran of 60-70 L exceeded the volume of total body water indicating moderate tissue distribution of dabigatran.
Biotransformation: Metabolism and excretion of dabigatran were studied following a single intravenous dose of radiolabeled dabigatran in healthy male subjects. After an intravenous dose, the dabigatran-derived radioactivity was eliminated primarily in the urine (85 %). Faecal excretion accounted for 6 % of the administered dose. Recovery of the total radioactivity ranged from 88-94 % of the administered dose by 168 hours post dose.
Dabigatran is subject to conjugation forming pharmacologically active acylglucuronides. Four positional isomers, 1-O, 2-O, 3-O, 4-O-acylglucuronide exist, each accounts for less than 10 % of total dabigatran in plasma. Traces of other metabolites were only detectable with highly sensitive analytical methods. Dabigatran is eliminated primarily in the unchanged form in the urine, at a rate of approximately 100 mL/min corresponding to the glomerular filtration rate.
Elimination: Plasma concentrations of dabigatran showed a biexponential decline with a mean terminal half-life of 11 hours in healthy elderly subjects. After multiple doses a terminal half-life of about 12-14 hours was observed. The half-life was independent of dose. Half-life is prolonged if renal function is impaired as shown in Table 12.
Special populations: Renal insufficiency: In phase I studies the exposure (AUC) of dabigatran after the oral administration of Pradaxa is approximately 2.7-fold higher in volunteers with moderate renal insufficiency (CrCL between 30-50 mL/min) than in those without renal insufficiency.
In a small number of volunteers with severe renal insufficiency (CrCL 10-30 mL/min), the exposure (AUC) to dabigatran was approximately 6 times higher and the half-life approximately 2 times longer than that observed in a population without renal insufficiency (see Dosage & Administration, Contraindications and Precautions). (See Table 12.)
Click on icon to see table/diagram/image
Additionally, dabigatran exposure (at trough and peak) was assessed in a prospective open label randomized pharmacokinetic study in NVAF patients with severe renal impairment (defined as creatinine clearance [CrCl] 15-30 mL/min) receiving dabigatran etexilate 75 mg twice daily.
This regimen resulted in a geometric mean trough concentration of 155 ng/ml (gCV of 76.9 %), measured immediately before administration of the next dose and in a geometric mean peak concentration of 202 ng/ml (gCV of 70.6 %) measured two hours after the administration of the last dose.
Clearance of dabigatran by haemodialysis was investigated in 7 patients with end-stage renal disease (ESRD) without atrial fibrillation. Dialysis was conducted with 700 mL/min dialysate flow rate, four hour duration and a blood flow rate of either 200 mL/min or 350-390 mL/min. This resulted in a removal of 50 % to 60 % of dabigatran concentrations, respectively. The amount of substance cleared by dialysis is proportional to the blood flow rate up to a blood flow rate of 300 mL/min. The anticoagulant activity of dabigatran decreased with decreasing plasma concentrations and the PK/PD relationship was not affected by the procedure.
The median CrCL in RE-LY was 68.4 mL/min. Almost half (45.8 %) of the RE-LY patients had a CrCL > 50-< 80 mL/min. Patients with moderate renal impairment (CrCL between 30-50 mL/min) had on average 2.29-fold and 1.81-fold higher pre- and post-dose dabigatran plasma concentrations, respectively, when compared with patients without renal impairment (CrCL ≥ 80 mL/min).
The median CrCL in the RE-COVER study was 100.4 mL/min. 21.7 % of patients had mild renal impairment (CrCL > 50 - < 80 mL/min) and 4.5% of patients had a moderate renal impairment (CrCL between 30 and 50 mL/min). Patients with mild and moderate renal impairment had at steady state an average 1.8-fold and 3.6-fold higher pre-dose dabigatran plasma concentrations compared with patients with CrCL > 80 mL/min, respectively. Similar values for CrCL were found in RE-COVER II.
The median CrCL in the RE-MEDY and RE-SONATE studies were 99.0 mL/min and 99.7 mL/min, respectively. 22.9 % and 22.5 % of the patients had a CrCL > 50-< 80 mL/min, and 4.1 % and 4.8 % had a CrCL between 30 and 50 mL/min in the RE-MEDY and RE-SONATE studies.
Elderly patients: Specific pharmacokinetic phase I studies with elderly subjects showed an increase of 40 to 60 % in the AUC and of more than 25 % in C
max compared to young subjects.
The effect by age on exposure to dabigatran was confirmed in the RE-LY study with an about 31 % higher trough concentration for subjects ≥ 75 years and by about 22 % lower trough level for subjects < 65 years compared to subjects between 65 and 75 years (see Dosage & Administration and Precautions).
Hepatic impairment: No change in dabigatran exposure was seen in 12 subjects with moderate hepatic insufficiency (Child Pugh B) compared to 12 controls (see Dosage & Administration and Precautions).
Body weight: The dabigatran trough concentrations were about 20 % lower in patients with a body weight > 100 kg compared with 50-100 kg. The majority (80.8 %) of the subjects were in the ≥ 50 kg and < 100 kg category with no clear difference detected (see Dosage & Administration and Precautions). Limited clinical data in patients < 50 kg are available.
Gender: Active substance exposure in the primary VTE prevention studies was about 40 % to 50 % higher in female patients and no dose adjustment is recommended. In atrial fibrillation patients females had on average 30 % higher trough and post-dose concentrations. No dose adjustment is required (see Dosage & Administration).
Ethnic origin: No clinically relevant inter-ethnic differences among Caucasian, African-American, Hispanic, Japanese or Chinese patients were observed regarding dabigatran pharmacokinetics and pharmacodynamics.
Pharmacokinetic interactions: In vitro interaction studies did not show any inhibition or induction of the principal isoenzymes of cytochrome P450. This has been confirmed by
in vivo studies with healthy volunteers, who did not show any interaction between this treatment and the following active substances: atorvastatin (CYP3A4), digoxin (P-gp transporter interaction) and diclofenac (CYP2C9).
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity and genotoxicity.
Effects observed in the repeated dose toxicity studies were due to the exaggerated pharmacodynamic effect of dabigatran.
An effect on female fertility was observed in the form of a decrease in implantations and an increase in pre-implantation loss at 70 mg/kg (5-fold the plasma exposure level in patients). At doses that were toxic to the mothers (5- to 10-fold the plasma exposure level in patients), a decrease in foetal body weight and viability along with an increase in foetal variations were observed in rats and rabbits. In the pre- and post-natal study, an increase in foetal mortality was observed at doses that were toxic to the dams (a dose corresponding to a plasma exposure level 4-fold higher than observed in patients).
In lifetime toxicology studies in rats and mice, there was no evidence for a tumorigenic potential of dabigatran up to maximum doses of 200 mg/kg.
Dabigatran, the active moiety of dabigatran etexilate mesilate, is persistent in the environment.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image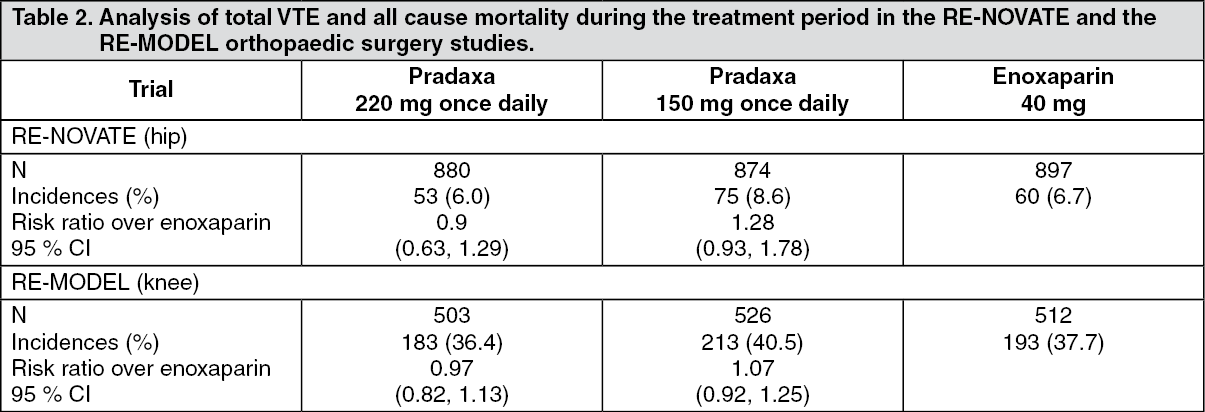 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image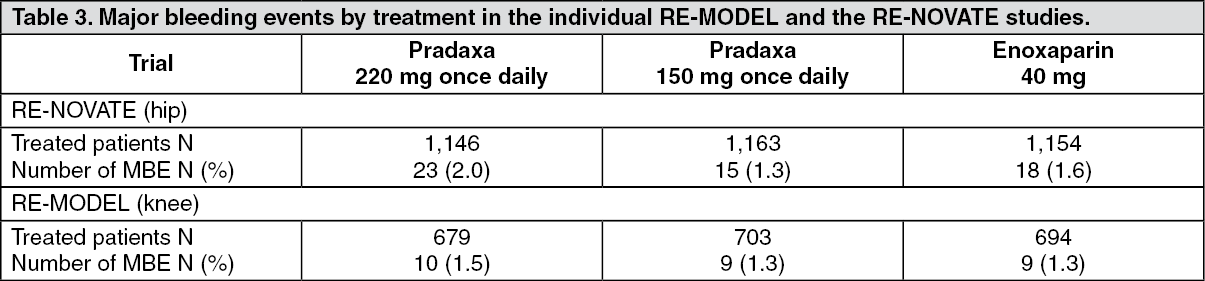 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image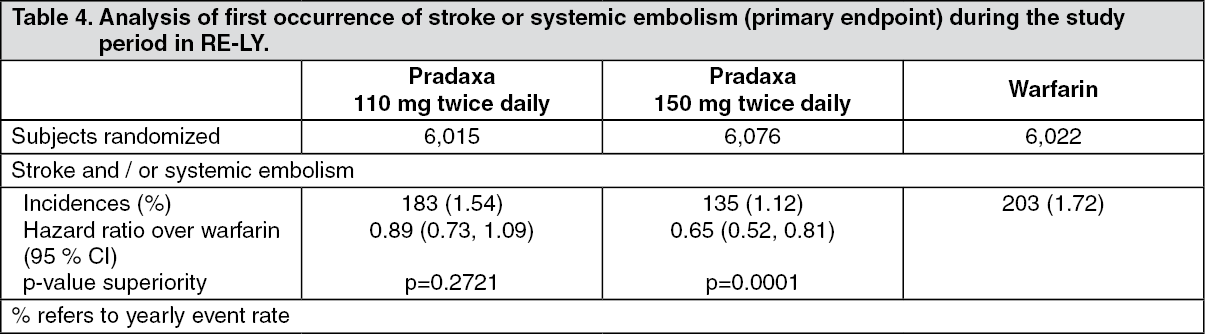 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image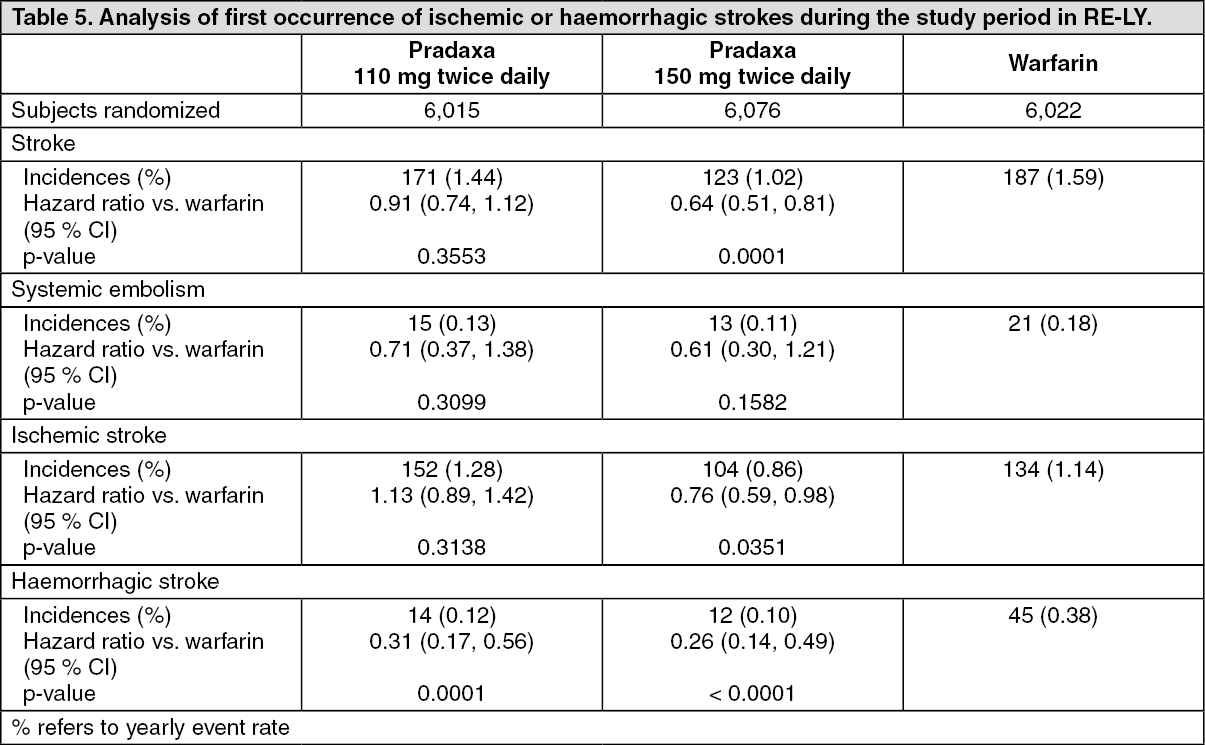 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image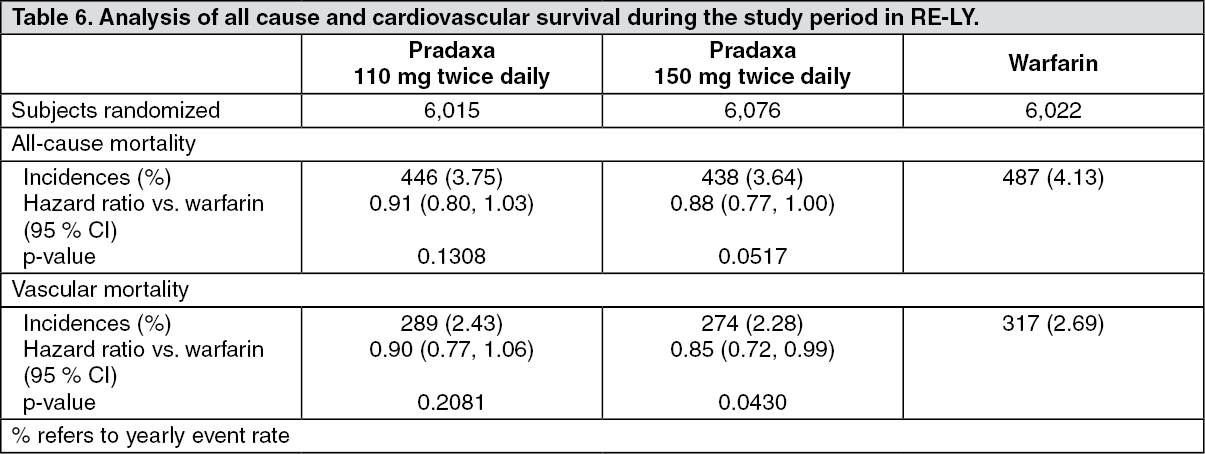 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image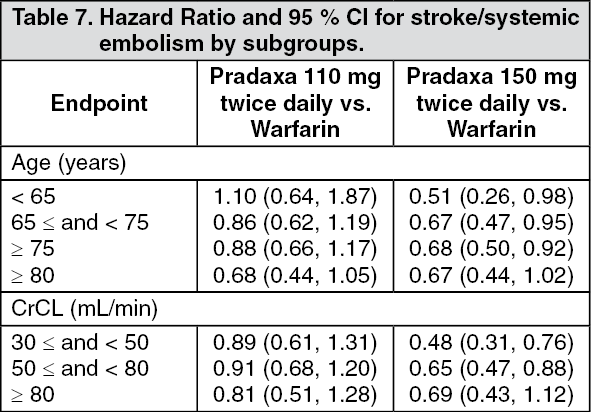 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image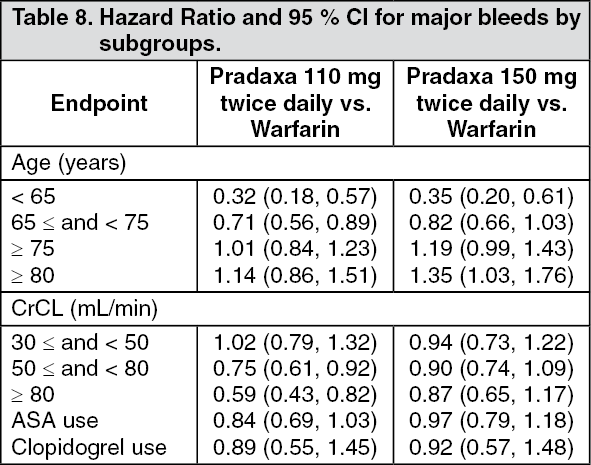 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image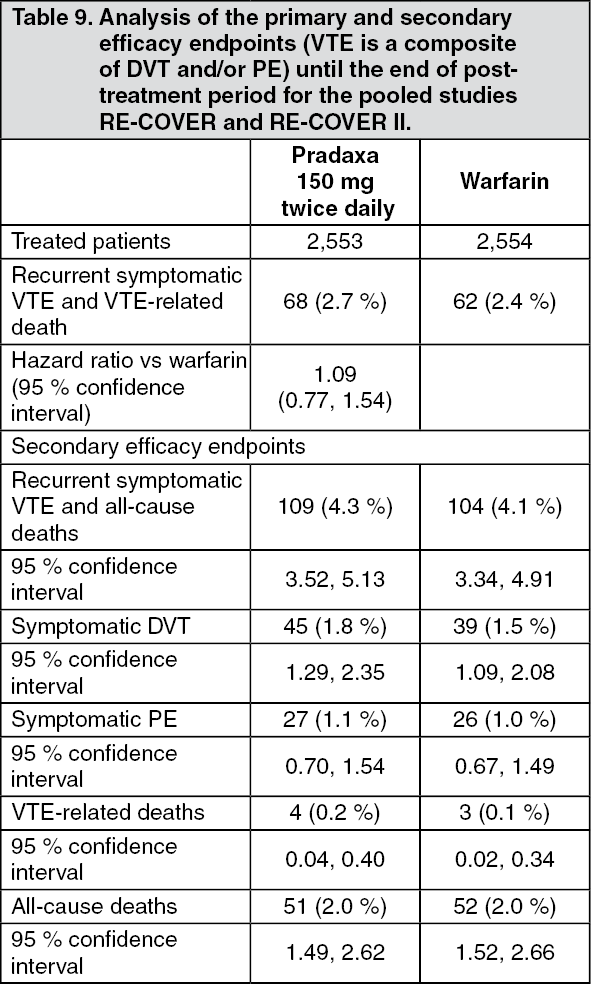 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image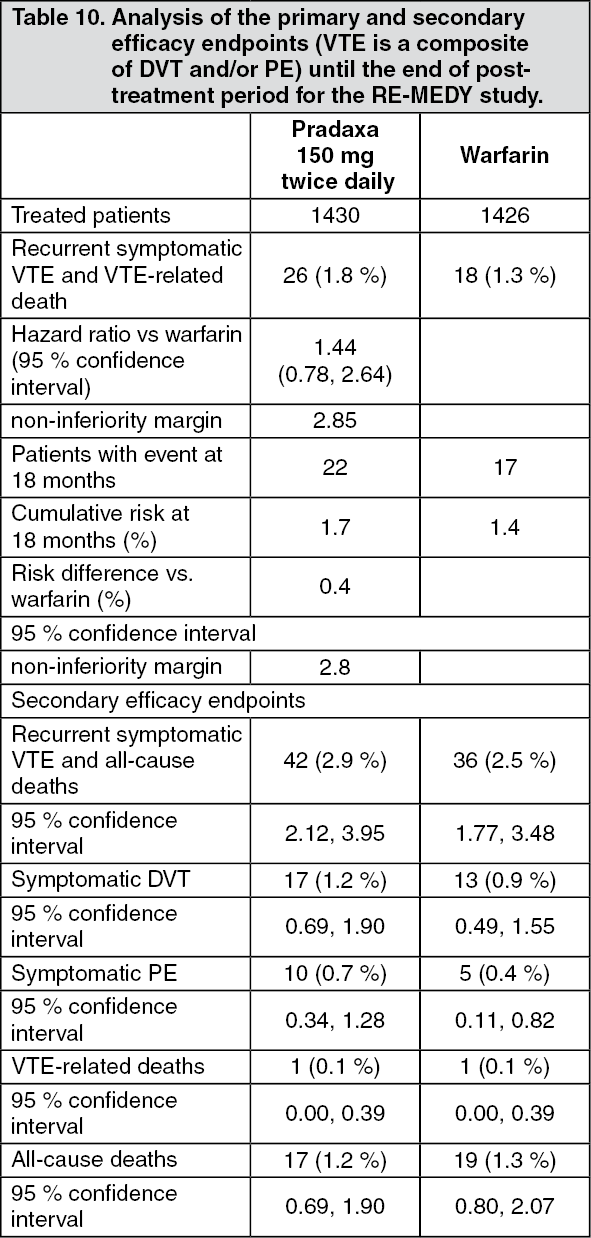 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image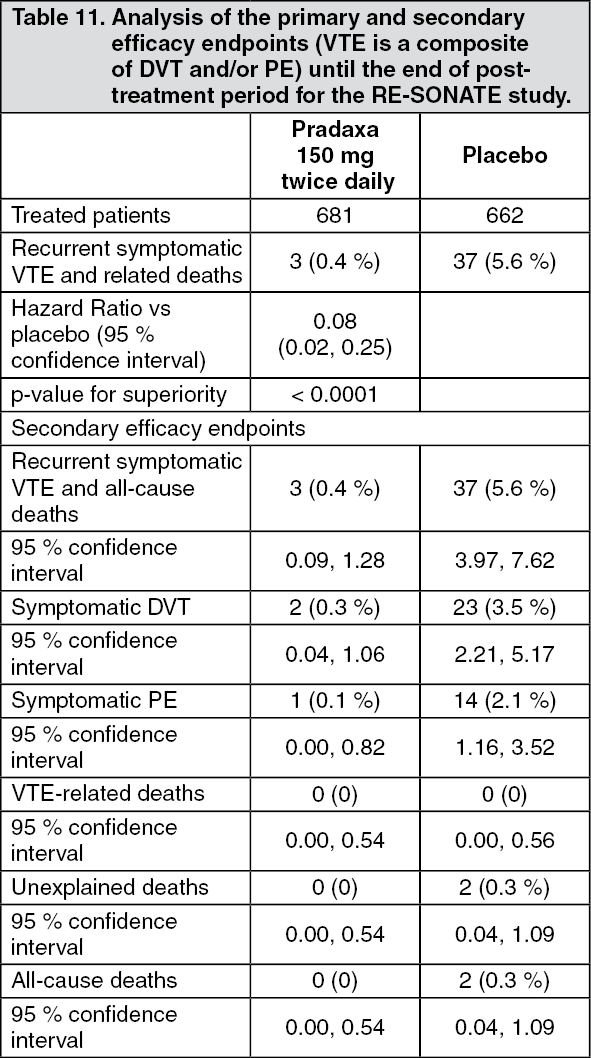 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image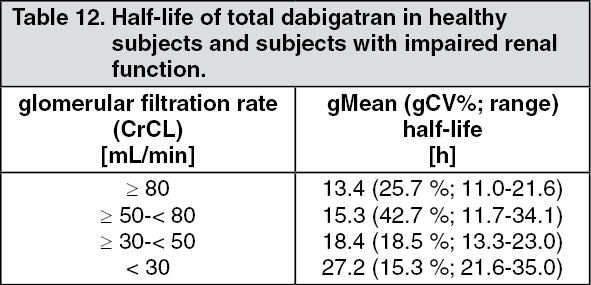 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image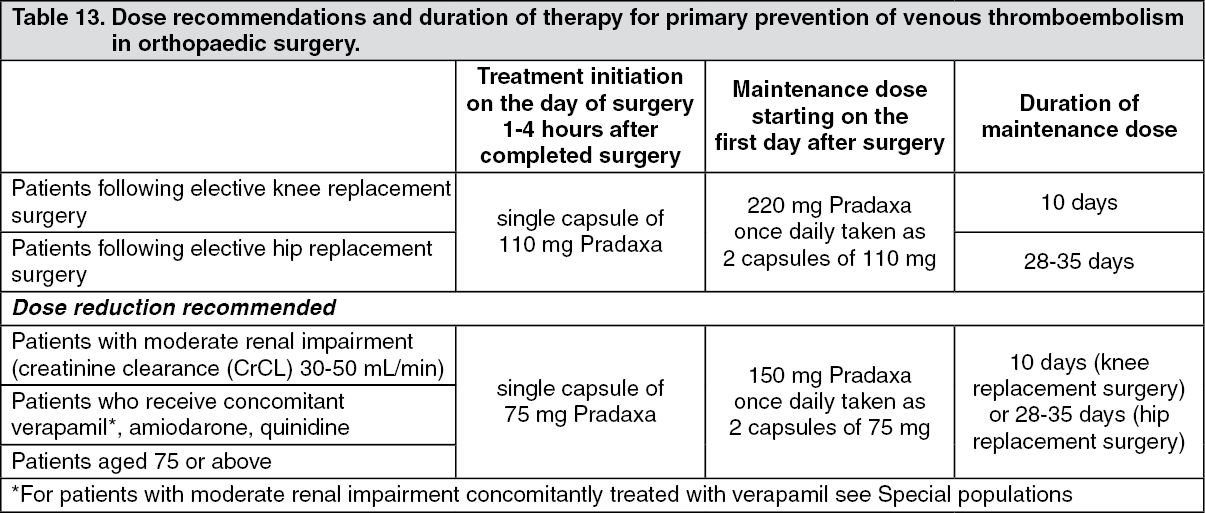 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image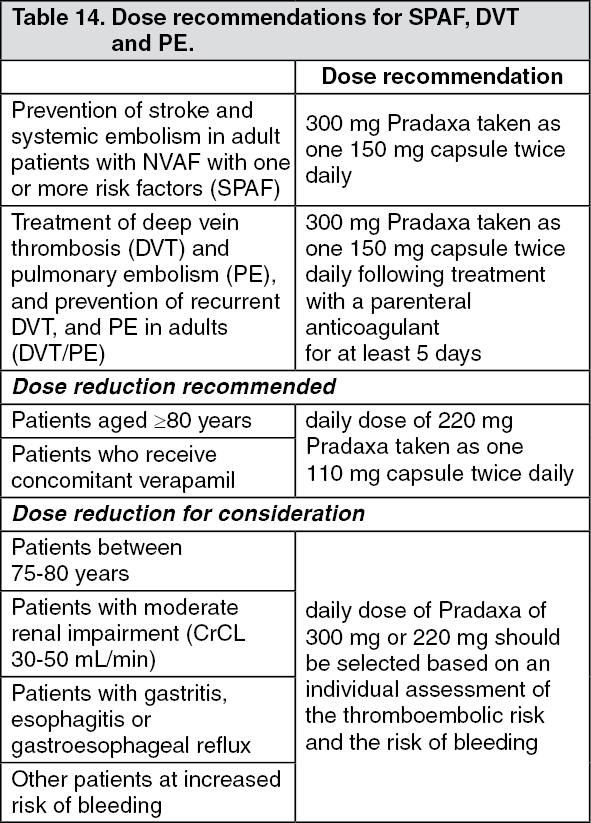 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image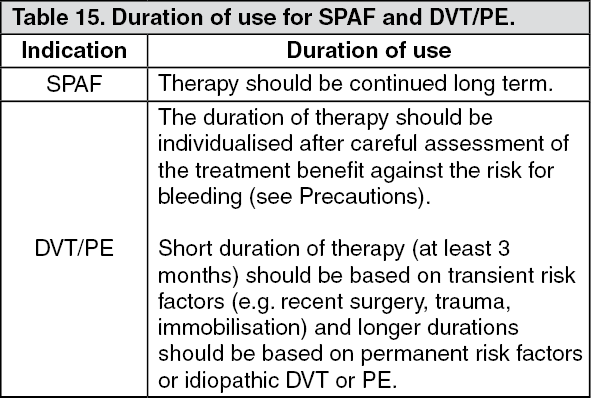 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image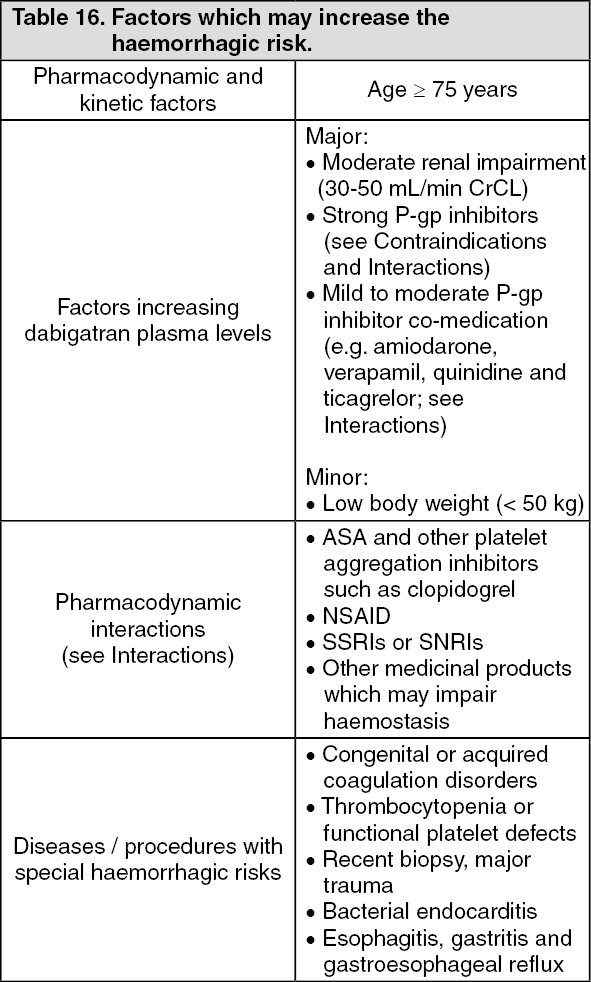 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image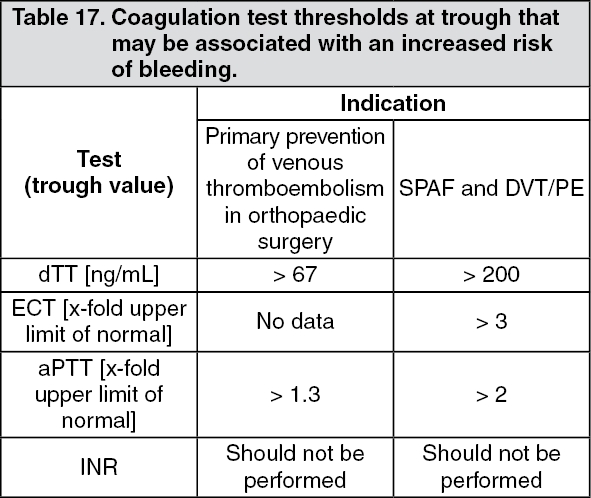 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image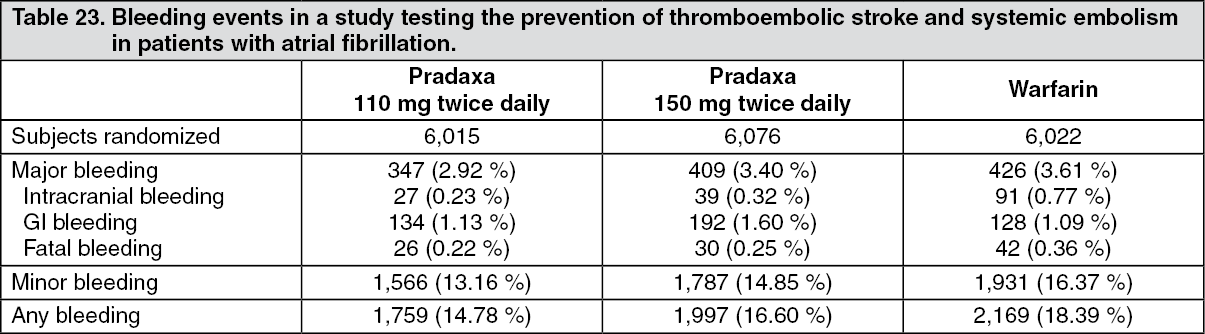 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image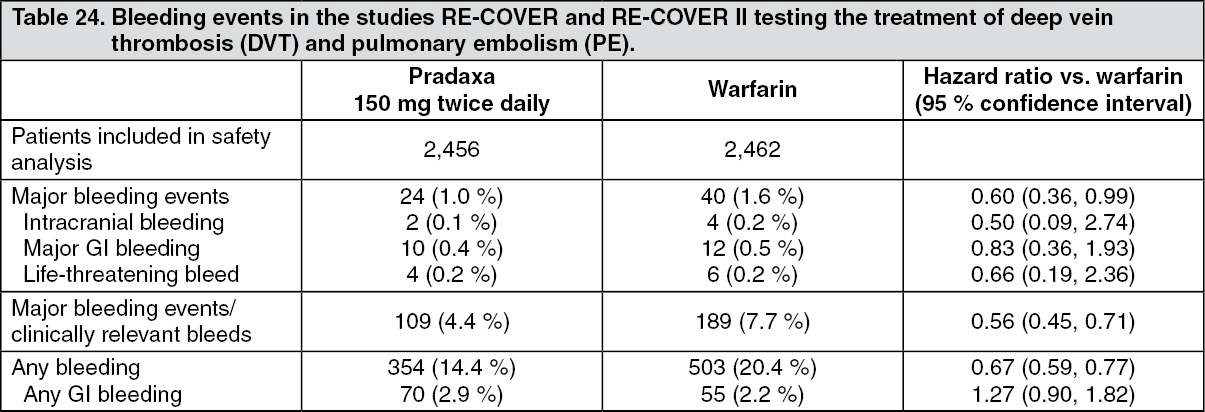 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image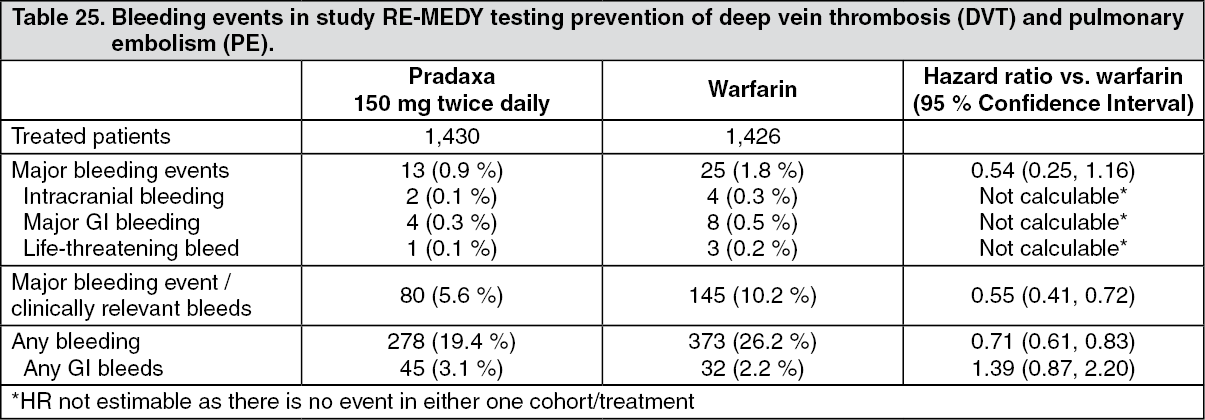 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image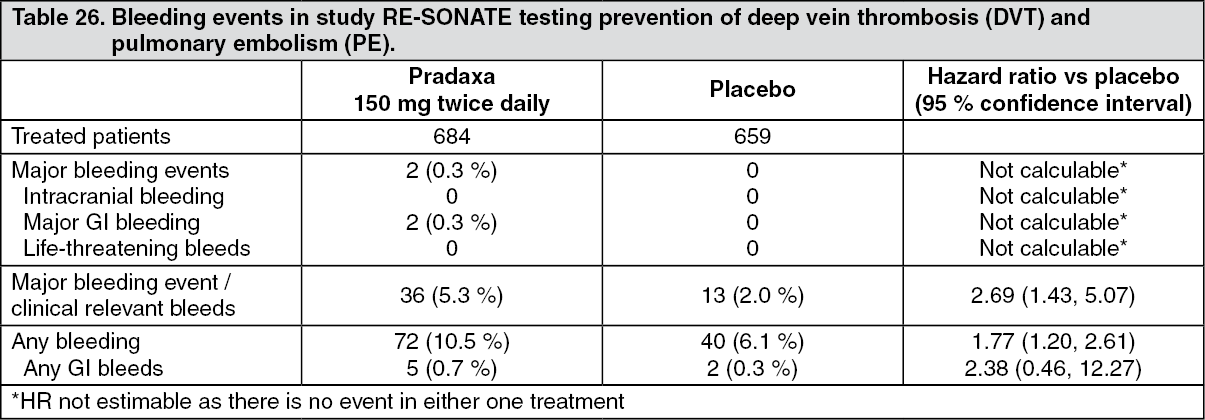 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
