Pharmacology: Pharmacodynamics: Mechanism of Action: Salmeterol is a selective long-acting (12 hour) beta-2-adrenoceptor agonist with a long side chain which binds to the exo-site of the receptor.
Pharmacodynamic Effects: These pharmacological properties of salmeterol offer more effective protection against histamine-induced bronchoconstriction and produce a longer duration of bronchodilation, lasting for at least 12 hours, than recommended doses of conventional short-acting beta-2 agonists.
In vitro tests have shown salmeterol is a potent and long-lasting inhibitor of the release from the human lung of mast cell mediators, such as histamine, leukotrienes and prostaglandin D
2. In man salmeterol inhibits the early and late phase response to inhaled allergen; the latter persisting for over 30 hours after a single dose when the bronchodilator effect is no longer evident. Single dosing with salmeterol attenuates bronchial hyper-responsiveness. These properties indicate that salmeterol has additional non-bronchodilator activity, but the full clinical significance is not yet clear. The mechanism is different from the anti-inflammatory effect of corticosteroids which should not be stopped or reduced when salmeterol is prescribed.
Salmeterol has been studied in the treatment of conditions associated with COPD and has been shown to improve symptoms, pulmonary function and quality of life.
In vitro salmeterol has also been shown to increase cilial beat frequency of human bronchial epithelial cells and also reduce a ciliotoxic effect of Pseudomonas toxin on the bronchial epithelium of patients with cystic fibrosis.
Clinical Studies: Asthma: The Salmeterol Multi-center Asthma Research Trial (SMART) was a large US study that compared the safety of SEREVENT or placebo added to usual therapy. There were no significant differences in the primary endpoint of the combined number of respiratory-related deaths and respiratory-related life-threatening experiences. The study showed a significant increase in asthma-related deaths in patients receiving SEREVENT (13 deaths out of 13,176 patients treated for 28 weeks on SEREVENT, versus, 3 deaths out of 13,179 patients on placebo). The study was not designed to assess the impact of concurrent inhaled corticosteroid use. However, post-hoc analyses showed there was no significant difference between treatment groups for asthma-related deaths for those patients using inhaled steroids at baseline (4/6127 on SEREVENT versus 3/6138 on placebo). The numbers of asthma-related deaths in the groups not using inhaled steroids were 9/7049 on SEREVENT versus 0/7041 on placebo. (See Tables 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Salmeterol acts locally in the lung therefore plasma levels are not an indication of therapeutic effects. In addition there are only limited data available on the pharmacokinetics of salmeterol because of the technical difficulty of assaying the drug in plasma due to the low plasma concentrations at therapeutic doses (approximately 200 picogram/ml or less) achieved after inhaled dosing.
In a placebo-controlled, crossover drug interaction study in 15 healthy subjects, coadministration of SEREVENT (50 micrograms twice daily inhaled) and the CYP3A4 inhibitor ketoconazole (400 mg once daily orally) for 7 days resulted in a significant increase in plasma salmeterol exposure (1.4-fold C
max and 15-fold AUC). There was no increase in salmeterol accumulation with repeat dosing. Three subjects were withdrawn from SEREVENT and ketoconazole co-administration due to QTc prolongation or palpitations with sinus tachycardia. In the remaining 12 subjects, co-administration of SEREVENT and ketoconazole did not result in a clinically significant effect on heart rate, blood potassium or QTc duration (see Precautions and Interactions).
Absorption: After regular dosing with salmeterol xinafoate, hydroxynaphthoic acid can be detected in the systemic circulation, reaching steady state concentrations of approximately 100 nanograms/ml. These concentrations are up to 1000 fold lower than steady state levels observed in toxicity studies and in long term regular dosing (more than 12 months) in patients with airways obstruction, have been shown to produce no ill effects.
Metabolism: An
in vitro study showed that salmeterol is extensively metabolised to α-hydroxysalmeterol (aliphatic oxidation) by cytochrome P450 3A4 (CYP3A4). A repeat dose study with salmeterol and erythromycin in healthy volunteers showed no clinically significant changes in pharmacodynamic effects at 500 mg three times daily doses of erythromycin. However, a salmeterol-ketoconazole interaction study resulted in a significant increase in plasma salmeterol exposure. (See Precautions and Interactions.)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image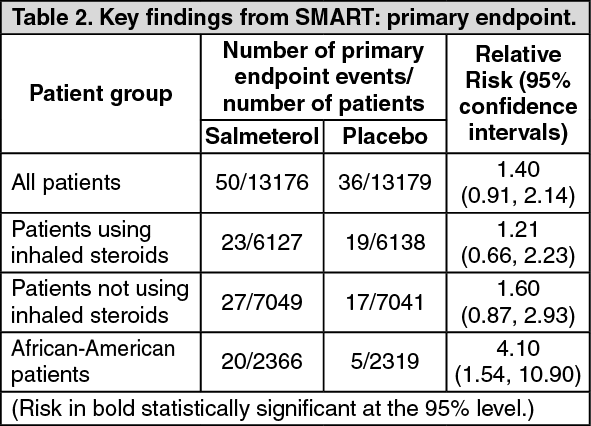 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image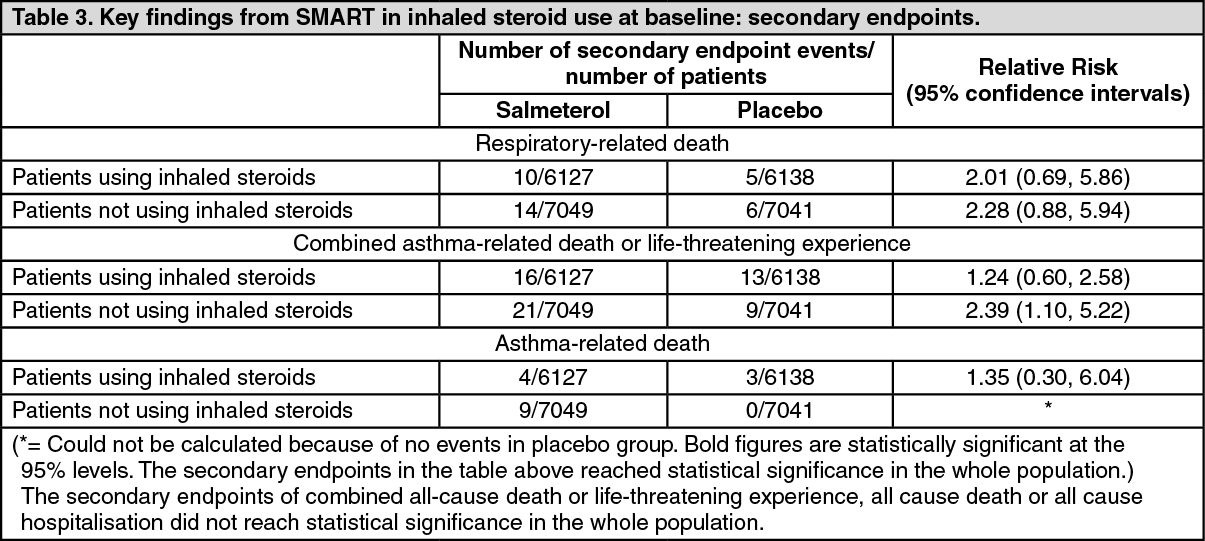 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
