


 Sign Out
Sign Out
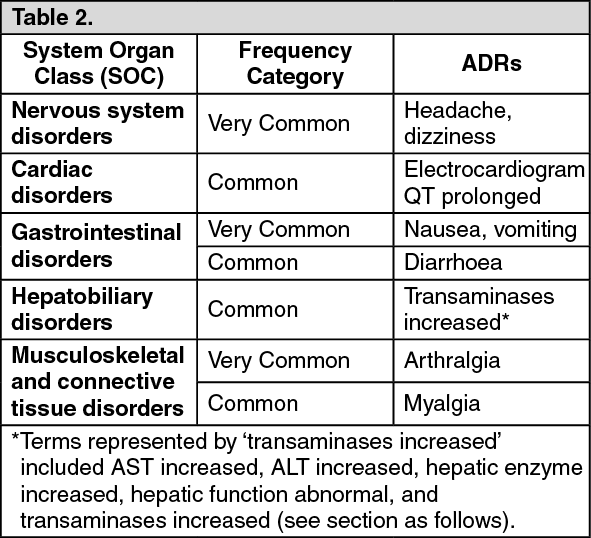
Tabulated list of adverse reactions: Adverse drug reactions to SIRTURO reported from controlled trials in 102 patients treated with SIRTURO are presented in the table as follows.
Adverse drug reactions are listed by system organ class (SOC) and frequency. Frequency categories are defined as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10) and uncommon (≥ 1/1,000 to < 1/100). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse events: Deaths: In the randomised phase IIb study (C208, stage 2) a higher rate of deaths was seen in the SIRTURO treatment group (12.7%;10/79 patients) compared to the placebo treatment group (3.7%; 3/81 patients). One death in the SIRTURO group and one death in the placebo group were reported after the week 120 window. In the SIRTURO group, all of the five deaths due to tuberculosis occurred in patients whose sputum culture status at last visit was 'not converted'. The causes of death in the remaining SIRTURO subjects were alcohol poisoning, hepatitis/hepatic cirrhosis, septic shock/peritonitis, cerebrovascular accident and motor vehicle accident. One of the ten deaths in the SIRTURO group (due to alcohol poisoning) occurred during the 24-week treatment period. The other nine deaths among those treated with SIRTURO occurred after completion of treatment with this agent (range 86-911 days post-SIRTURO; median 344 days). The observed imbalance in deaths between the two treatment groups is unexplained. No discernible pattern between death and sputum culture conversion, relapse, sensitivity to other medicinal products used to treat tuberculosis, human immunodeficiency virus status, or severity of disease could be observed. During the trial, there was no evidence of antecedent significant QT prolongation or clinically significant dysrhythmia in any of the patients that died.
In the Phase IIb, open-label study (C209), 6.9% (16/233) patients died. The most common cause of death as reported by the investigator was tuberculosis (9 patients). All but one patients who died of tuberculosis had not converted or had relapsed. The causes of death in the remaining patients varied.
Description of selected adverse reactions: Cardiovascular: In the controlled Phase IIb study (C208), mean increases from baseline values in QTcF were observed from the first on-treatment assessment onwards (9.9 ms at week 1 for SIRTURO and 3.5 ms for placebo). The largest mean increase from baseline values in QTcF during the 24 weeks of SIRTURO treatment was 15.7 ms (at week 18). After the end of SIRTURO treatment (i.e. after week 24), QTcF increases in the SIRTURO group gradually became less pronounced. The largest mean increase from baseline values in QTcF in the placebo group during the first 24 weeks was 6.2 ms (also at week 18) (see Precautions).
In the Phase IIb, open label study (C209), where patients with no treatment options received other QT-prolonging medicinal products used to treat tuberculosis, including clofazimine, concurrent use with SIRTURO resulted in additive QT prolongation, proportional to the number of QT prolonging medicinal products in the treatment regimen.
Patients receiving SIRTURO alone with no other QT prolonging medicinal product developed a maximal mean QTcF increase over baseline of 23.7 ms with no QT duration in excess of 480 ms, whereas patients with at least 2 other QT prolonging medicinal products developed a maximal mean QTcF prolongation of 30.7 ms over baseline, resulting in a QTcF duration in excess of 500 ms in one patient.
There were no documented cases of Torsade de Pointes in the safety database (see Precautions). See Interactions, QT interval and concomitant clofazimine use, for further information regarding patients using clofazimine concomitantly.
Increased transaminases: In study C208 (stage 1 and 2), aminotransferase elevations of at least 3 x ULN developed more frequently in the SIRTURO treatment group (11/102 [10.8%] versus 6/105 [5.7%]) in the placebo treatment group. In the SIRTURO treatment group, the majority of these increases occurred throughout the 24 weeks of treatment and were reversible. During the investigational phase in Stage 2 of study C208, increased aminotransferases were reported in 7/79 (8.9%) patients in the SIRTURO treatment group compared to 1/81 (1.2%) in the placebo treatment group.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form