


 Sign Out
Sign Out
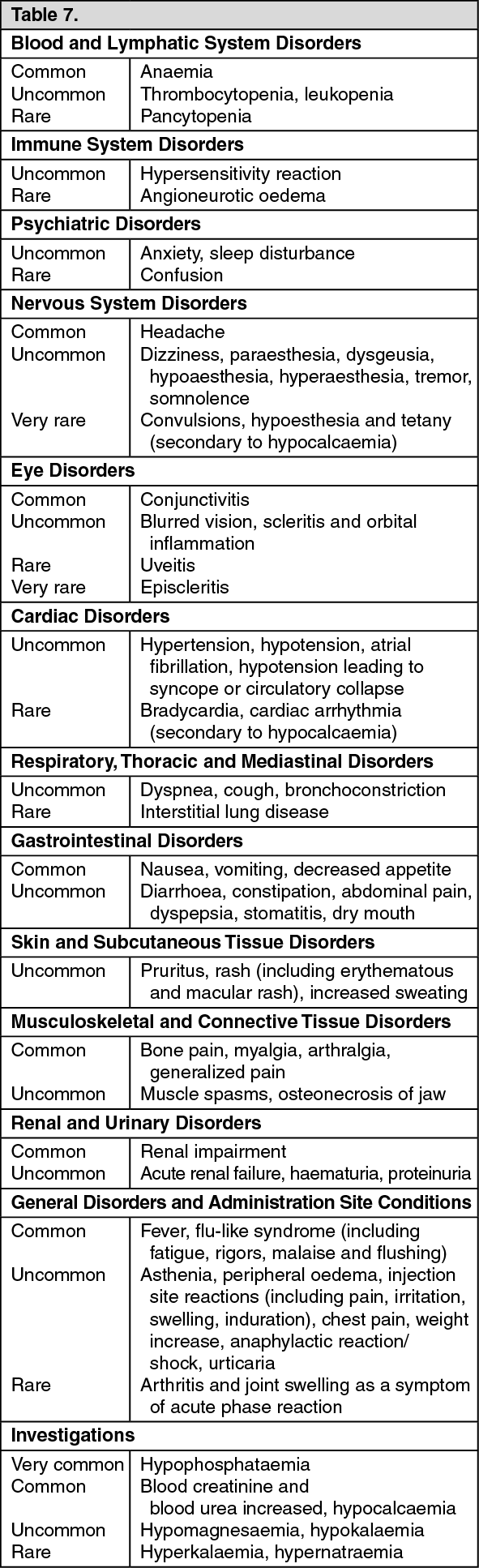
The following are the important identified risks with Zometa in the approved indications: Renal function impairment, osteonecrosis of the jaw, acute phase reaction, hypocalcaemia, atrial fibrillation, anaphylaxis, interstitial lung disease. The frequencies for each of these identified risks are shown in Table 7.
Tabulated list of adverse reactions: The following adverse reactions, listed in Table 7, have been accumulated from clinical studies and post-marketing reports following predominantly chronic treatment with 4 mg zoledronic acid.
Adverse reactions are ranked under headings of frequency, the most frequent first, using the following convention: Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Renal function impairment: Zometa has been associated with reports of renal dysfunction. In a pooled analysis of safety data from Zometa registration trials for the prevention of skeletal-related events in patients with advanced malignancies involving bone, the frequency of renal impairment adverse events suspected to be related to Zometa (adverse reactions) was as follows: multiple myeloma (3.2%), prostate cancer (3.1%), breast cancer (4.3%), lung and other solid tumours (3.2%). Factors that may increase the potential for deterioration in renal function include dehydration, pre-existing renal impairment, multiple cycles of Zometa or other bisphosphonates, as well as concomitant use of nephrotoxic medicinal products or using a shorter infusion time than currently recommended. Renal deterioration, progression to renal failure and dialysis have been reported in patients after the initial dose or a single dose of 4 mg zoledronic acid (see Precautions).
Osteonecrosis of the jaw: Cases of osteonecrosis of the jaw have been reported, predominantly in cancer patients treated with medicinal products that inhibit bone resorption, such as Zometa (see Precautions). Many of these patients were also receiving chemotherapy and corticosteroids and had signs of local infection including osteomyelitis. The majority of the reports refer to cancer patients following tooth extractions or other dental surgeries.
Atrial fibrillation: In one 3-year, randomised, double-blind controlled trial that evaluated the efficacy and safety of zoledronic acid 5 mg once yearly vs. placebo in the treatment of postmenopausal osteoporosis (PMO), the overall incidence of atrial fibrillation was 2.5% (96 out of 3,862) and 1.9% (75 out of 3,852) in patients receiving zoledronic acid 5 mg and placebo, respectively. The rate of atrial fibrillation serious adverse events was 1.3% (51 out of 3,862) and 0.6% (22 out of 3,852) in patients receiving zoledronic acid 5 mg and placebo, respectively. The imbalance observed in this trial has not been observed in other trials with zoledronic acid, including those with Zometa (zoledronic acid) 4 mg every 3-4 weeks in oncology patients. The mechanism behind the increased incidence of atrial fibrillation in this single clinical trial is unknown.
Acute phase reaction: This adverse drug reaction consists of a constellation of symptoms that includes fever, myalgia, headache, extremity pain, nausea, vomiting, diarrhoea arthralgia and arthritis with subsequent joint swelling. The onset time is ≤ 3 days post-Zometa infusion, and the reaction is also referred to using the terms "flu-like" or "post-dose" symptoms.
Atypical fractures of the femur: During post-marketing experience the following reactions have been reported (frequency rare): Atypical subtrochanteric and diaphyseal femoral fractures (bisphopsphonate class adverse reaction).
Hypocalcaemia-related ADRs: Hypocalcaemia is an important identified risk with Zometa in the approved indications. Based on the review of both clinical trial and post-marketing cases, there is sufficient evidence to support an association between Zometa therapy, the reported event of hypocalcaemia, and the secondary development of cardiac arrhythmia. Furthermore, there is evidence of an association between hypocalcaemia and secondary neurological events reported in these cases including; convulsions, hypoaesthesia and tetany (see Precautions).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form