Ziprasidone hydrochloride monohydrate.
Ziprasidone is available as capsules for oral administration: 40 mg – No. 4 blue capsules, marked "Pfizer" and "ZDX 40".
60 mg – No. 3 white capsules, marked "Pfizer" and "ZDX 60".
Capsules containing ziprasidone hydrochloride monohydrate equivalent to 40 or 60 mg ziprasidone.
Excipients/Inactive Ingredients: Lactose monohydrate, pregelatinized maize starch, magnesium stearate, gelatin, titanium dioxide, indigotin.
Pharmacology: Pharmacodynamics: Receptor Binding Studies: Ziprasidone has a high affinity for dopamine type 2 (D2) receptors and substantially higher affinity for serotonin type 2A (5HT2A) receptors. Ziprasidone also interacts with serotonin 5HT2C, 5HT1D and 5HT1A receptors where its affinities for these sites are equal to or greater than its affinity for the D2 receptor. Ziprasidone has moderate affinity for neuronal serotonin and norepinephrine transporters. Ziprasidone demonstrates moderate affinity for histamine H1- and alpha1-receptors. Antagonism at these receptors has been associated with somnolence and orthostatic hypotension, respectively. Ziprasidone demonstrates negligible affinity for muscarinic M1-receptors. Antagonism at this receptor has been associated with memory impairment.
Receptor Functional Studies: Ziprasidone has been shown to be an antagonist at both serotonin type 2A (5HT2A) and dopamine type 2 (D2) receptors. It is proposed that the antipsychotic activity is mediated, in part, through this combination of antagonist activities.
Ziprasidone is also a potent antagonist at 5HT2C and 5HT1D receptors, a potent agonist at the 5HT1A receptor and inhibits neuronal reuptake of norepinephrine and serotonin.
Human PET Studies: At 12 hours following a 40 mg oral dose of ziprasidone, receptor blockade was greater than 80% for 5HT2A and greater than 50% for D2 using positron emission tomography (PET).
Further Information from Clinical Trials: In a double-blind comparative study, metabolic parameters including weight, fasting levels of total cholesterol, triglycerides, insulin and an insulin resistance (IR) index were measured. In patients receiving ziprasidone no significant changes from baseline were observed in any of these metabolic parameters.
Results of a Large Post-Marketing Safety Study: A randomized post-approval study of 18,239 patients with observational follow-up for 1 year was conducted to determine whether ziprasidone's effect on the QTc interval is associated with an increased risk of non-suicide mortality in patients with schizophrenia. This study, which was conducted in naturalistic clinical practice settings, showed no difference in the rate of non-suicide mortality between ziprasidone and olanzapine treatments.
Pharmacokinetics: Following oral administration of multiple doses of ziprasidone with food, peak serum concentrations typically occur 6 to 8 hours post-dose. Ziprasidone demonstrates linear kinetics over the therapeutic dose range of 40-80 mg twice daily in fed subjects.
The absolute bioavailability of a 20 mg dose is 60% in the fed state. The absorption of ziprasidone is reduced by up to 50% when ziprasidone is administered under fasting conditions. In a multiple dose study, ziprasidone oral suspension was shown to be bioequivalent to ziprasidone capsules under steady-state conditions. In a single dose administration study, bioequivalence was demonstrated with regard to AUC. A slightly lower Cmax was achieved with oral suspension than with capsules.
Twice daily dosing generally leads to attainment of steady state within three days. Systemic exposures at steady state are related to dose.
At steady-state, the mean terminal elimination half-life of ziprasidone is about 6.6 hours following oral dosing. Mean systemic clearance of ziprasidone administered intravenously is 7.5 mL/min/kg and the volume of distribution is approximately 1.5 L/kg. Ziprasidone is extensively bound (>99%) to plasma proteins and its binding appears to be independent of concentration.
Ziprasidone is extensively metabolized after oral administration with only a small amount (<1%) excreted in urine or feces (<4%) as unchanged drug. Ziprasidone is primarily cleared via three metabolic routes to yield four major circulating metabolites, benzisothiazole piperazine (BITP) sulphoxide, BITP sulphone, ziprasidone sulphoxide and S-methyl-dihydroziprasidone. Approximately 20% of the dose is excreted in urine, with approximately 66% being eliminated in feces. Unchanged ziprasidone represents about 44% of total drug-related material in serum.
Ziprasidone is primarily metabolized by two pathways: reduction and methylation to generate S-methyl-dihydroziprasidone which accounts for approximately two-thirds of the metabolism, and oxidative metabolism accounting for the other third. In vitro studies using human liver subcellular fractions indicate that S-methyl-dihydroziprasidone is generated in two steps. These studies indicate that the first step is mediated primarily by chemical reduction by glutathione as well as by enzymatic reduction by aldehyde oxidase. The second step is methylation mediated by thiol methyltransferase. In vitro studies indicate that CYP3A4 is the major cytochrome P450 catalyzing the oxidative metabolism of ziprasidone.
Ziprasidone, S-methyl-dihydroziprasidone, and ziprasidone sulphoxide, when tested in vitro, share properties which may predict a QTc-prolonging effect. S-methyl-dihydroziprasidone is mainly eliminated by fecal excretion and CYP3A4 catalyzed metabolism. The sulphoxide is eliminated through renal extraction and by secondary metabolism catalyzed by CYP3A4.
In a phase I trial, the CYP3A4 inhibitor ketoconazole (400 mg/day) increased the serum concentrations of ziprasidone by <40%. The serum concentration of S-methyl-dihydroziprasidone, at the expected Tmax of ziprasidone, was increased by 55% during ketoconazole treatment. No additional QTc prolongation was observed.
No clinically significant differences in the pharmacokinetics of ziprasidone in young and elderly male or female subjects were observed following oral administration.
Pharmacokinetic screening of patients treated orally has not revealed any significant pharmacokinetic differences between smokers and non-smokers.
No marked differences in the pharmacokinetics of oral ziprasidone have been observed in patients with moderate to severe impairments in renal function as compared to subjects with normal renal function. It is unclear whether serum concentrations of the metabolites are increased in these patients.
In mild to moderate impairment of liver function (Child-Pugh A or B), the serum concentrations of ziprasidone after oral administration were 30% higher and the terminal half-life was about two hours longer than in normal subjects.
Toxicology: Preclinical Safety Data: Preclinical safety data on ziprasidone revealed no special hazard for humans based on conventional studies of safety pharmacology, genotoxicity and carcinogenic potential. In reproductive studies in rats and rabbits, ziprasidone has shown no evidence of teratogenicity. Adverse effects on fertility and increased numbers of pups born dead, decreased pup weights and delayed functional development were observed at doses that caused adverse effects suggestive of maternal toxicity (e.g., sedation, decreased body weight gain). Increased perinatal mortality and delayed functional development of offspring occurred at maternal plasma concentrations extrapolated to be similar to the maximal concentrations in humans given therapeutic doses.
Schizophrenia: Ziprasidone is indicated for the management of schizophrenia and other psychotic disorders and for maintenance of clinical improvement and prevention of relapse during continuation therapy.
The efficacy of ziprasidone in the treatment of the positive and negative symptoms of schizophrenia was established in four- and six-week placebo- and active-controlled clinical trials of hospitalized patients experiencing an acute exacerbation of the illness.
In a 52-week placebo-controlled clinical trial of chronic stable inpatients, ziprasidone demonstrated continuing improvement in primary negative symptoms and in global (psychological, social and occupational) functioning in this study of inpatient population over a 52-week period.
An analysis of the effect of ziprasidone on patients with clinically significant depressive symptoms, defined as ≥14 on the Montgomery-Asberg Depression Rating Scale (MADRS), was conducted in two multicenter placebo-controlled studies in acute schizophrenia. A statistically significant improvement versus placebo (p <0.05) in the MADRS was observed in these two studies in patients receiving 60 mg and 80 mg twice daily.
Bipolar Mania: Ziprasidone is indicated for the treatment of manic or mixed episodes associated with bipolar disorder, with or without psychotic features.
Treatment of mania with ziprasidone for more than 3 weeks and prophylactic use in bipolar disorder have not been systematically evaluated in controlled clinical trials.
Bipolar I Disorder: Ziprasidone is indicated as monotherapy for the acute treatment of manic or mixed episodes associated with bipolar I disorder. Efficacy was established in two 3-week monotherapy studies in adult patients.
Ziprasidone is indicated as an adjunct to lithium or valproate for the maintenance treatment of bipolar I disorder. Efficacy was established in a maintenance trial in adult patients. The efficacy of Ziprasidone as monotherapy for the maintenance treatment of bipolar I disorder has not been systematically evaluated in controlled clinical trials.
Use of Ziprasidone Capsules: For oral use. Capsules should be taken with food and swallowed whole without chewing, crushing or opening beforehand..
Use in Adults: Schizophrenia and Bipolar Mania: The recommended initial dose is 40 mg twice daily, to be taken with food (See Pharmacology: Pharmacokinetics under Actions). Daily dosage may subsequently be adjusted on the basis of individual clinical status up to a maximum of 80 mg twice daily. If indicated, the maximum recommended dose may be reached as early as Day 3 of treatment.
Use in Children: Safety and effectiveness in children under 18 years have not been established.
Use in the Elderly: Generally, no dosage adjustment is required in elderly patients (65 years and over).
Use in Renal Impairment: No dosage adjustment is required in patients with renal impairment.
Use in Hepatic Impairment: In patients with mild to moderate hepatic insufficiency, lower doses should be considered. There is a lack of experience in patients with severe hepatic insufficiency and ziprasidone should be used with caution in this group (See Pharmacology: Pharmacokinetics under Actions).
Use in Smokers: No dosage adjustment is required in patients who smoke.
Bipolar I Disorder: Acute Treatment of Manic or Mixed Episodes: The recommended initial dose is 40 mg twice daily, to be taken with food. Daily dosage may subsequently be adjusted on the basis of individual clinical status up to a maximum of 80 mg twice daily. If indicated, the maximum recommended dose may be reached as early as Day 3 of treatment.
Maintenance Treatment (as an adjunct to lithium or valproate): Continue treatment at the same dose on which the patient was initially stabilized, within the range of 40 mg - 80 mg twice daily with food. Patients should be periodically reassessed to determine the need for maintenance treatment.
Experience with ziprasidone overdosage is limited. The largest confirmed single ingestion is 12,800 mg. In this case, extrapyramidal symptoms and a QTc interval of 446 msec (with no cardiac sequelae) were reported. In overdose cases in general, the most commonly reported symptoms are extrapyramidal symptoms, somnolence, tremor, and anxiety.
There is no specific antidote to ziprasidone. In cases of acute overdosage, establish and maintain an airway and ensure adequate ventilation and oxygenation. Gastric lavage (after intubation, if patient is unconscious) and administration of activated charcoal, together with a laxative, should be considered. The possibility of obtundation, seizures or dystonic reaction of the head and neck following overdose may create a risk of aspiration with induced emesis. Cardiovascular monitoring should commence immediately and should include continuous electrocardiographic monitoring to detect possible arrhythmias. Given the high protein binding of ziprasidone, hemodialysis is unlikely to be beneficial in the treatment of overdose. Close medical monitoring and supervision should continue until the patient recovers.
Ziprasidone is contraindicated in patients with: Known hypersensitivity to ziprasidone or any of the excipients; Known QT-interval prolongation including congenital long QT Syndrome; Recent myocardial infarction; Uncompensated heart failure; Cardiac arrhythmias requiring treatment with Class IA and III antiarrhythmic drugs (See Precautions).
QT Interval: Ziprasidone causes a mild to moderate prolongation of the QT interval.
In the pre-marketing clinical trials database, the incidence of QTc prolongation above 500 msec was 3 in a total of 3266 (0.1%) in ziprasidone-treated patients and 1 in a total of 538 (0.2%) in placebo-treated patients.
Some drugs including Class IA and III antiarrhythmics that prolong the QT interval greater than 500 msec have been associated with the rare occurrence of Torsade de pointes, a life-threatening arrhythmia (See Contraindications).
There have been rare post-marketing reports of torsade de pointes in patients with multiple confounding risk factors taking ziprasidone. A causal relationship with ziprasidone has not been established.
Ziprasidone should be used with caution in patients with the following risk factors, which can increase the risk for occurrence of this arrhythmia: bradycardia; electrolyte imbalance; concomitant use with other drugs that prolong QT.
If cardiac symptoms suggestive of arrhythmias are observed or reported during treatment, then appropriate cardiac diagnostics should be performed. If the QTc interval is greater than 500 msec, it is recommended that treatment be stopped (See Contraindications).
Venous Thromboembolism: Cases of venous thromboembolism (VTE) have been reported with antipsychotic drugs. Since patients treated with antipsychotics often present with acquired risk factors for VTE, all possible risk factors for VTE should be identified before and during treatment with ziprasidone and preventive measures undertaken.
Neuroleptic Malignant Syndrome (NMS): Neuroleptic Malignant Syndrome (NMS), a potentially fatal complex, has been reported in association with antipsychotic drugs, including ziprasidone. If a patient develops signs and symptoms indicative of NMS, or presents with unexplained high fever without additional clinical manifestations of NMS, all antipsychotic drugs must be discontinued.
Severe Cutaneous Adverse Reactions: Drug reaction with eosinophilia and systemic symptoms (DRESS) has been reported with ziprasidone exposure. DRESS consists of a combination of three or more of the following: cutaneous reaction (such as rash or exfoliative dermatitis), eosinophilia, fever, lymphadenopathy and one or more systemic complications, such as hepatitis, nephritis, pneumonitis, myocarditis, and pericarditis.
Other severe cutaneous adverse reactions, such as Stevens-Johnson syndrome, have been reported with ziprasidone exposure.
Severe cutaneous adverse reactions are sometimes fatal. Discontinue ziprasidone if severe cutaneous adverse reactions occur.
Tardive Dyskinesia: There is a potential for ziprasidone to cause tardive dyskinesia and other tardive extrapyramidal syndromes after long-term treatment. If signs and symptoms of tardive dyskinesia appear, dose reduction or discontinuation of ziprasidone should be considered.
Falls: Antipsychotic drugs (which includes ziprasidone) may cause somnolence, postural hypotension, and motor and sensory instability, which could lead to falls and, consequently, fractures or other injuries. For patients with diseases, conditions, or medications that could exacerbate these effects, a fall risk assessment should be completed when initiating antipsychotic treatment and recurrently for patients on long-term antipsychotic therapy.
Seizures: Caution is recommended when treating patients with a history of seizures.
CNS Drugs/Alcohol: Given the primary CNS effects of ziprasidone, caution should be used when it is taken in combination with other centrally acting agents, including alcohol and drugs acting on the dopaminergic and serotonergic systems.
Medicinal Products Containing Lactose: As the capsule contains the excipient lactose (See Description), patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Increased Risk of Cerebrovascular Accidents in the Dementia Population: An approximately 3-fold increased risk of cerebrovascular adverse events has been seen in randomized placebo-controlled clinical trials in the dementia population with some atypical antipsychotics. The mechanism for this increased risk is not known. An increased risk cannot be excluded for other antipsychotics or other patient populations. Zeldox should be used with caution in patients with risk factors for stroke.
Increased Mortality in Elderly Patients with Dementia-related Psychosis: Elderly patients with dementia-related psychosis have been shown to be at an increased risk of death and/or potentially, cerebrovascular adverse events compared with placebo when treated with some antipsychotic drugs. Study data with ziprasidone in the treatment of elderly patients with dementia are insufficient to conclude whether or not there is an increased risk of death with ziprasidone versus placebo in this patient population. Ziprasidone is not approved for the treatment of elderly patients with dementia-related psychosis.
Priapism: Cases of priapism have been reported with antipsychotic use, including ziprasidone. This adverse reaction, as with other psychotropic drugs, did not appear to be dose-dependent and did not correlate with the duration of treatment.
Hyperprolactinemia: As with other drugs that antagonize dopamine D2 receptors, ziprasidone may elevate prolactin levels. Disturbances, such as galactorrhea, amenorrhea, gynecomastia, and impotence have been reported with prolactin-elevating compounds. Long-standing hyperprolactinemia when associated with hypogonadism may lead to decreased bone density.
Hyperglycemia/Diabetes Mellitus: Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse events is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycemia-related adverse events in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse events in patients treated with atypical antipsychotics are not available.
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g. obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patients treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia and weakness.
Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
Effects on Ability to Drive and Use Machines: Ziprasidone may cause somnolence. Patients should be cautioned about operating hazardous machinery, including automobiles, until they are reasonably certain that ziprasidone does not affect them adversely.
Use in Pregnancy: No studies have been conducted in pregnant women. Women of childbearing potential receiving ziprasidone should therefore, be advised to use an appropriate method of contraception. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress and feeding disorder in these neonates. These complications have varied in severity; while in some cases symptoms have been self-limited, in other cases neonates have required intensive care unit support and prolonged hospitalization.
Ziprasidone should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus (See Pharmacology: Toxicology: Preclinical Safety Data under Actions).
Use in Lactation: There are no adequate and well-controlled studies in lactating women. Limited data indicate that ziprasidone is excreted into breast milk at very low levels. Patients should be advised not to breastfeed if they are receiving ziprasidone.
Fertility: There are no adequate and well-controlled studies in women and men exposed to ziprasidone.
Contraception - Women of childbearing potential receiving ziprasidone should be advised to use an appropriate method of contraception.
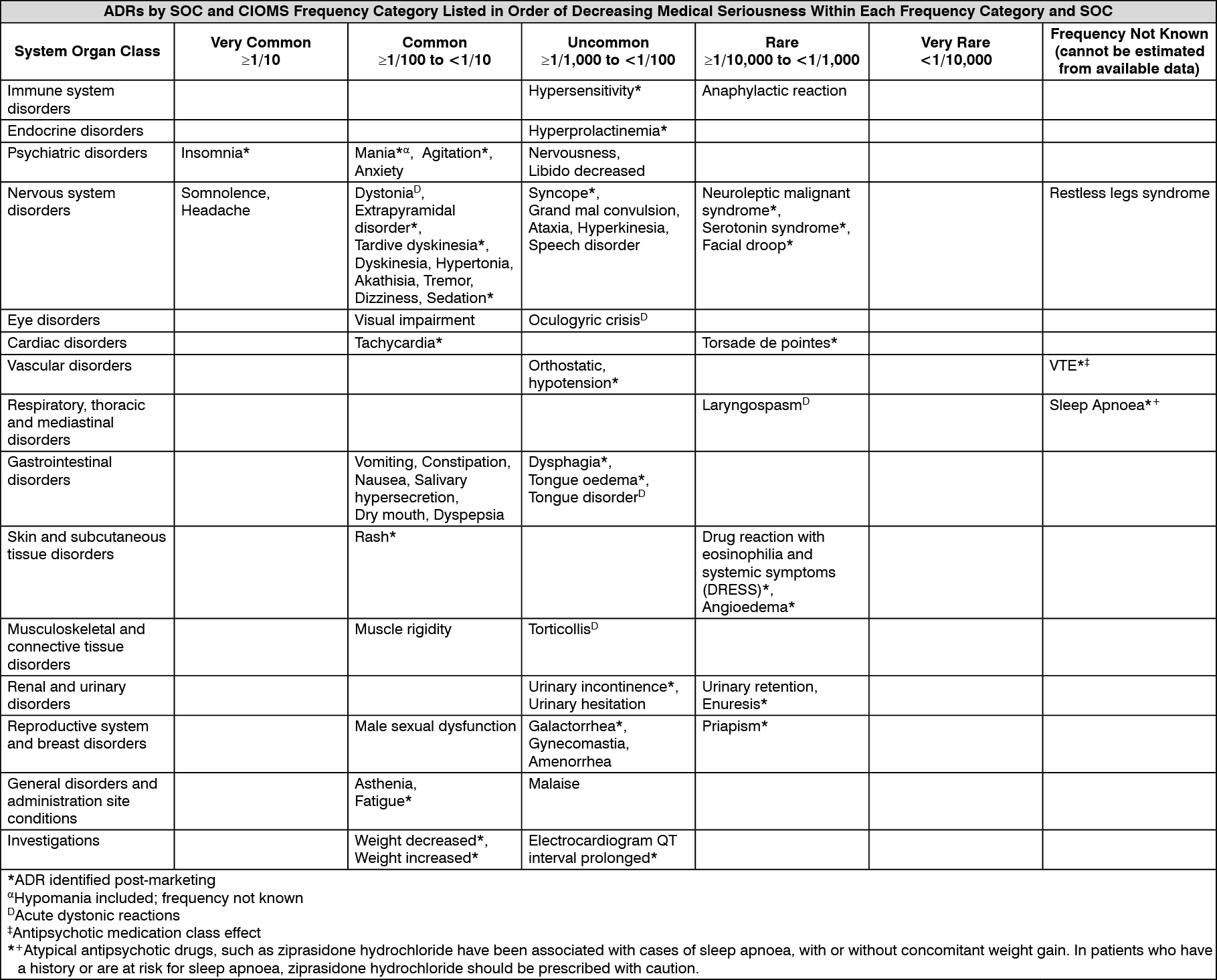
Adverse drug reactions reported from clinical trials and post-marketing experience include: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Class IA and III Antiarrhythmic Drugs (See Contraindications and QT Interval under Precautions).
Concomitant use with other drugs that prolong QT Interval (See QT Interval under Precautions).
CNS Drugs/Alcohol (See CNS Drugs/Alcohol under Precautions).
Effect of Ziprasidone on Other Drugs: Using human liver microsomes, ziprasidone demonstrated no inhibitory effect on CYP1A2, CYP2C9 or CYP2C19. The concentration of ziprasidone required to inhibit CYP2D6 and CYP3A4 in vitro is at least 1000-fold higher than the free concentration that can be expected in vivo.
Dextromethorphan - Consistent with in vitro results, a study in normal healthy volunteers showed that ziprasidone did not alter the CYP2D6 mediated metabolism of dextromethorphan to its major metabolite, dextrorphan.
Oral Contraceptives - Ziprasidone administration results in no significant change to the pharmacokinetics of estrogen (ethinyl estradiol, a CYP3A4 substrate) or progesterone components.
Lithium - Co-administration of ziprasidone has no effect on the pharmacokinetics of lithium.
Protein binding - Ziprasidone extensively binds to plasma proteins. The in vitro plasma protein binding of ziprasidone was not altered by warfarin or propranolol, two highly protein-bound drugs, nor did ziprasidone alter the binding of these drugs in human plasma. Thus, the potential for drug interactions with ziprasidone due to displacement is unlikely.
Effects of Other Drugs on Ziprasidone: In vitro and animal data suggest that ziprasidone may be a P-glycoprotein (P-gp) substrate. The in vivo relevance for humans remains unknown.
Ketoconazole (400 mg/day), a potent inhibitor of CYP3A4, which also inhibits P-gp, produced an increase of approximately 35% in ziprasidone exposure (AUC and Cmax). Since ziprasidone is a substrate of CYP3A4 and induction of CYP3A4 and P-gp is related, co-administration with inducers of CYP3A4 and P-gp, such as carbamazepine, rifampin and St. John's Wort could cause decreased concentrations of ziprasidone. Carbamazepine 200 mg twice daily, an inducer of CYP3A4, produced a decrease of 36% in ziprasidone exposure.
Cimetidine, a nonspecific CYP inhibitor, did not significantly affect ziprasidone pharmacokinetics.
Antacid - Multiple doses of aluminium- and magnesium-containing antacids did not affect the pharmacokinetics of ziprasidone.
Incompatibilities (major): None known.
Special Precautions for Disposal and Other Handling: No special requirements.
N05AE04 - ziprasidone ; Belongs to the class of indole derivatives antipsychotics.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
