Ampicillin sodium, sulbactam sodium.
Each 750 mg Powder for Injection contains: Ampicillin (as sodium) equivalent to Ampicillin 500 mg, Sulbactam (as sodium) equivalent to Sulbactam 250 mg.
Each 1.5 g Powder for Injection contains: Ampicillin (as sodium) equivalent to Ampicillin 1 g, Sulbactam (as sodium) equivalent to Sulbactam 500 mg.
Pharmacotherapeutic group: Antibacterial for systemic use.
Pharmacology: Pharmacodynamics: Mechanism of action: Ampicillin acts through the inhibition of the biosynthesis of the cell wall mucopeptide. Ampicillin has a broad spectrum of bactericidal action against many Gram-positive and Gram-negative aerobic and anaerobic bacteria, but is degraded by β-lactamases. Many β-lactamases found in microorganisms resistant to penicillins and to cephalosporins are irreversibly inhibited by Sulbactam, which alone has a little useful bactericidal activity. Beta-lactamase inhibition by Sulbactam is a two-step process. Initially, Sulbactam reversibly forms an inactive enzyme-inhibitor complex with beta-lactamase. In a time- and concentration-dependent manner, this complex evolves into one, or more, irreversibly inactivated proteins. Sulbactam's ability to protect resistant microorganisms against their degradation by penicillins and cephalosporins has been confirmed in all in vivo studies using resistant strains. In these studies Sulbactam showed a synergic activity with penicillins and cephalosporins. Since Sulbactam is bound to certain equal binding sites of penicillin-binding proteins, some susceptible strains are even more susceptible to this combination than to beta-lactam antibiotics alone. Pharmacodynamic effects, Ampicillin and Sulbactam is a combination of a beta-lactam antibiotic (Ampicillin) and an irreversible beta-lactamase inhibitor (Sulbactam). Sulbactam alone has a very poor antibacterial activity which is of very little utility except against the Neisseriaceae, Acinetobacter calcoaceticus, Bacteroides spp, Branhamella catarrhalis and Pseudomonas cepacia but the combination with Ampicillin restores the activity of Ampicillin against β-lactamase producing strains. The combination, for parenteral use only, has a broad spectrum antibacterial activity against gram-positive and gram-negative aerobic and anaerobic bacteria including beta-lactamase producing strains.
Pharmacokinetics: General: Peak serum levels are achieved within 15 minutes after completion of I.V. infusion or after 30-60 minutes following I.M. administration. Serum concentrations are dependent upon the dose of the drug used, the route and body weight of the patient. The mean serum half-life of both drugs is approximately one hour in healthy volunteers. Approximately 75 to 85% of both Sulbactam and Ampicillin are excreted unchanged in the urine during the first 8 hours after administration to individuals with normal renal function. In patients with impaired renal function, the elimination kinetics of Sulbactam and Ampicillin are similarly affected, hence the ratio of one to the other remains constant whatever the renal function is. The dose of Sulbactam Sodium/Ampicillin Sodium in such patients should be administered in accordance with the usual practice for Ampicillin. Ampicillin is approximately 28% reversibly bound to human serum protein and Sulbactam is approximately 38% reversibly bound. It penetrates readily into the various tissues and body fluids like peritoneal fluid, intestinal mucosa, appendix etc. and offers synergistic bactericidal concentration. Penetration of both Sulbactam and Ampicillin into cerebrospinal fluid in the presence of inflamed meninges has been demonstrated after IV administration.
Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Long-term studies in animals have not been performed to evaluate carcinogenic or mutagenic potential.
Microbiology: A wide range of beta-lactamase found in microorganisms resistant to penicillins and cephalosporins have been shown to be irreversibly inhibited by Sulbactam. Although Sulbactam alone possesses little useful antibacterial activity, it is effective against the Neisseriaceae. Whole organism studies have shown that Sulbactam restores Ampicillin's activity against beta-lactamase producing strains. In particular, Sulbactam has good inhibitory activity against the clinically important plasmid mediated beta-lactamase most frequently responsible for transferred drug resistance. Sulbactam has no deleterious effect on the activity of Ampicillin against Ampicillin susceptible strains.
The presence of Sulbactam in the formulation effectively extends the antimicrobial spectrum of ampicillin to include many bacteria normally resistant to it and to other beta-lactam antibiotics. Thus, it possesses the synergistic properties of broad-spectrum antibiotic and beta-lactamase inhibitor.
The bacterial activity of Ampicillin has a broad spectrum bactericidal activity against many Gram-positive and Gram-negative aerobic and anaerobic bacteria. Ampicillin is, however, degraded by beta-lactamase and therefore, the spectrum of activity does not normally include beta-lactamase producing organisms.
Susceptible microorganisms: Gram-positive Bacteria: Staphylococcus aureus (beta-lactamase and non-beta-lactamase producing), Streptococcus epidermis (beta-lactamase and non-beta-lactamase producing), Streptococcus saprophyticus (beta-lactamase and non-beta-lactamase producing), Streptococcus faecalis* (Enterococcus), Streptococcus pneumoniae* (formerly D. pneumoniae), Streptococcus pyogenes*, Streptococcus viridans*.
Gram-negative Bacteria: Haemophilus influenzae (beta-lactamase and non-beta-lactamase producing), Branhamella catarrhalis (formerly Neisseria catarrhalis) (beta-lactamase and non-beta-lactamase producing), Klebsiella species (all known strains are beta-lactamase producing), Proteus vulgaris, Morganella morganii and Neisseria gonorrhoeae (beta-lactamase and non-beta-lactamase producing).
Anaerobic: Bacteroides species, including B. fragilis. (*These are not beta-lactamase producing strains and therefore, are susceptible to ampicillin alone).
Used in the treatment of infections where beta-lactamase producing organisms might occur, including uncomplicated gonorrhoea, otitis media and respiratory tract and urinary tract infections.
It may be administered by either IV or the IM routes: For IV administration, the dose can be given by slow intravenous injection dissolved in 5 mL of sterile water for injection over at least 10-15 minutes or can be delivered in greater dilution with 50-100 mL of compatible diluent as an intravenous infusion over 15-30 minutes. It may be administered by deep intramuscular injection. The recommended daily dose is 1 vial 6-8 hours. The total daily dose of Sulbactam should not exceed 4 g/day. The duration of the treatment depends upon the severity of injection. For antibiotic prophylaxis in elective surgery, a different dosage regimen may be required or, as prescribed by the physician.
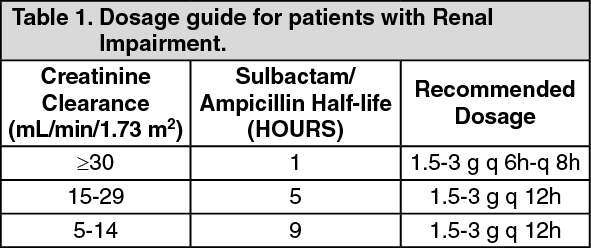
Impaired Renal Function: In patients with impairment of renal function, the elimination kinetics of Sulbactam and Ampicillin are similarly affected. Hence, the ratio of one to the other will remain constant whatever the renal function. The dose in such patients should be administered less frequently in accordance with the usual practice for ampicillin and according to the following recommendations. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
When only serum creatinine is available, the following formula (based on sex, weight and age of the patient) may be used to convert this value into creatinine clearance. The serum creatinine should represent a steady state of renal function. (See equation.)
Click on icon to see table/diagram/image
Neurological adverse reactions, including convulsions, may occur with the attainment of high CSF levels of beta-lactams. Ampicillin may be removed from circulation by hemodialysis. The molecular weight, degree of protein binding and pharmacokinetics profile of Sulbactam suggest that this compound may also be removed by hemodialysis.
It is contraindicated in patients with a history of hypersensitivity to any of the penicillins.
Serious and occasionally anaphylactic reactions have been reported in patients on penicillin therapy. These reactions occur in individuals with a history of penicillin hypersensitivity and/or hypersensitivity reactions to multiple allergens. There have been reports of individuals with a history of penicillin hypersensitivity that have experienced severe reactions when treated with Cephalosporins. Before therapy with penicillin, careful inquiry should be made concerning previous hypersensitivity reactions to resuscitation measures instituted.
Serious anaphylactoid reactions require immediate emergency treatment with Epinephrine, Oxygen, Intravenous steroids and airway management, including intubations should also be as indicated.
General: Ampicillin class of antibiotics should not be administered to patients with infectious mononucleosis. In patients, the possibility of superinfections with mycotic or bacterial pathogens should be kept in mind as with other beta-lactam antibiotics during therapy. If superinfections occur, the drug is discontinued and/or appropriate resuscitation measures instituted.
Pregnancy: Reproduction studies have been performed in mice, rats and rabbits at doses up to ten (10) times the human dose and have related no evidence of impaired fertility or harm to the fetus. There are however, no adequate and well controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Labor and Delivery: Studies in guinea pigs have shown that intravenous administration of Ampicillin decreased the uterine tone, height and duration of contraction. However, it is not known whether its use in human during labor or delivery has immediate or delayed adverse effects on the fetus, prolongs the duration of labor, or increases the likelihood that forceps delivery or other obstetrical intervention or resuscitation of the newborn will be necessary.
Nursing Mothers: Low concentrations of Sulbactam and Ampicillin are excreted in the milk, therefore, caution should be exercised when administered to a nursing mother.
It is generally well tolerated. The following adverse reactions have been reported.
Systemic Adverse Reaction: Adverse reactions were diarrhea in 3% of the patients and rash in less than 2% of the patients. Additional systemic reactions reported in literature in less than 1% of the patients were itching, nausea, vomiting, candidiasis, fatigue, malaise, headache, chest pain, flatulence, abdominal distension, glossitis, urine retention, dysuria, edema, facial swelling, erythema, chills, tightness in throat, substernal pain, epistaxis and mucosal bleeding.
The following adverse reactions have been reported with Ampicillin class antibiotics and can also occur with Sulbactam Sodium/Ampicillin Sodium.
Gastrointestinal: Gastritis, stomach, black hairy tongue, enterocolitis and pseudomembranous colitis. Occasionally, elevation in liver enzyme levels have been reported which revert to normal on discontinuation of the drug.
Hypersensitivity Reactions: Urticaria, erythema multiforme and occasional case of exfoliative dermatitis have been reported. These reactions may be controlled with antihistamines and if necessary systemic corticosteroids. Whenever such reactions occur, the drug should be discontinued, unless the opinion of the physician dictates otherwise. Serious and occasional fatal hypersensitivity (anaphylactic) reactions can occur with penicillin.
Hematologic: In addition to the adverse laboratory changes like fall in hemoglobin levels, hematocrit and increase in leukocyte count has been reported during therapy with penicillins. All of these reactions are usually reversible on discontinuation of therapy and are believed to be hypersensitivity phenomena.
Probenecid decreases the renal tubular secretion of Ampicillin and Sulbactam. Concurrent use together with probenecid may result in increased and prolonged blood levels of Ampicillin and Sulbactam.
The concurrent administration of allopurinol and Ampicillin increases substantially the incidence of rashes in patients receiving both drugs as compared to patients receiving Ampicillin alone. It is known whether this potentiation of Ampicillin rashes is due to allopurinol or the hyperuricemia present in these patients. There are no data with Ampicillin/Sulbactam and allopurinol administered concurrently. Combination with aminoglycoside should not be reconstituted together due to the in vitro inactivation of aminoglycosides by the Ampicillin component. Administration results in high urine concentration of ampicillin which gives rise to false positive reactions when testing for the presence of glucose in urine using Clinitest, Benedict's solution or Fehling's solution. Following administration of Ampicillin to pregnant women a transient decrease in plasma concentration of total conjugated estriol, estrioglucuronide, conjugated estrone and estradiol has been noted.
Compatibility, Reconstitution and Stability: To be stored at a temperature not exceeding 25°C prior to reconstitution. When concomitant therapy with aminoglycosides is indicated, combination with aminoglycosides should be reconstituted and administered separately, due to the
in vitro inactivation of aminoglycosides by any of the amino-penicillins.
Directions for Use: General Dissolution Procedure: Sterile powder for intravenous and intramuscular use may be reconstituted with any of the compatible diluents described in this monograph. Solutions should be allowed to stand after dissolution to allow any foaming to dissipate in order to permit visual inspection for complete solubilization.
Preparation for Intravenous use: Sterile powder may be reconstituted directly to the desired concentration using any of the following parenteral diluents. Reconstitution at the specified concentrations, with these diluents provides stable solutions for the time periods indicated in the following table. After the indicated time periods, any unused portions of solutions should be discarded. Initially the contents of vials may be dissolved in 3 mL of Sterile Water for Injection. This solution should be further diluted with an infusion medium to give a final concentration of around 15 to 30 mg/mL. The reconstituted solution should be infused over a period of 15 to 30 minutes.
Preparation for Intramuscular Use: The contents of 1.5 g vial should be reconstituted with 3 mL Sterile Water for Injection and for 0.75 g vial 2 mL of Sterile Water for Injection should be used.
NOTE: Use only freshly reconstituted solutions and administer within half hour after preparation. (There is sufficient excess present to allow withdrawal and administration of the stated volumes). Do not allow to freeze. (See Table 2.)
Click on icon to see table/diagram/image
Store at temperatures not exceeding 25°C. Protect from moisture.
J01CR01 - ampicillin and beta-lactamase inhibitor ; Belongs to the class of penicillin combinations, including beta-lactamase inhibitors. Used in the systemic treatment of infections.
Ampimax 1.5 g powd for inj
1's
Ampimax 750 mg powd for inj
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image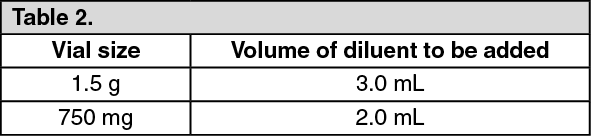 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out