


 Sign Out
Sign Out


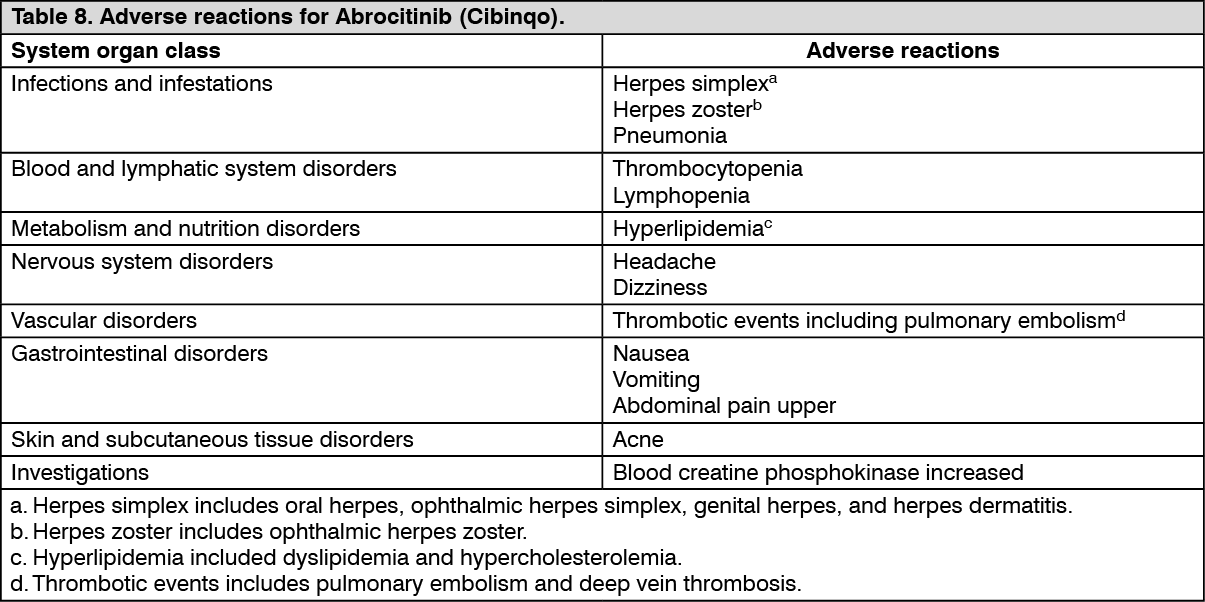
Tabulated list of adverse reactions: A total of 3582 patients were treated with Abrocitinib (Cibinqo) in clinical studies in atopic dermatitis, among them 2784 patients (representing 3006 patient-years of exposure) were integrated for safety analysis, 1451 patients with at least 48 weeks of exposure. The integrated safety analysis included 1761 patients receiving a constant dose of Abrocitinib 200 mg and 1023 patients receiving 100 mg. Five placebo-controlled studies were integrated (703 patients on 100 mg once daily, 684 patients on 200 mg once daily and 438 patients on placebo) to evaluate the safety of Abrocitinib (Cibinqo) in comparison to placebo for up to 16 weeks. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Infections: In placebo-controlled studies, for up to 16 weeks, overall infections have been reported in 27.4% of patients treated with placebo and in 34.9% and 34.8% of patients treated with Abrocitinib (Cibinqo) 100 mg and 200 mg, respectively. Most infections were mild or moderate.
The percentage of patients reporting infection-related adverse reactions in the 200 mg and 100 mg groups compared to placebo were: herpes simplex (4.2% and 2.8% versus 1.4%), herpes zoster (1.2% and 0.6% versus 0%), pneumonia (0.1% and 0.1% versus 0%). Herpes simplex was more frequent in patients with a history of herpes simplex or eczema herpeticum. Most of the herpes zoster events involved a single dermatome and were non-serious.
Among all patients treated with Abrocitinib in the integrated safety analysis, including the long-term extension study, the incidence rate of herpes zoster in patients treated with Abrocitinib 200 mg (4.83 per 100 patient-years) was higher than that of patients treated with 100 mg (2.39 per 100 patient-years). Incidence rates for herpes zoster were also higher for patients 65 years of age and older, patients with a medical history of herpes zoster, patients with severe atopic dermatitis at baseline, and a confirmed ALC <1.0 × 103/mm3 prior to the event of herpes zoster.
In placebo-controlled studies, for up to 16 weeks, the rate of serious infections was 1.81 per 100 patient-years in patients treated with placebo, 3.32 per 100 patient-years in patients treated with 100 mg, and 1.12 per 100 patient-years in patients treated with 200 mg. Among all patients treated with Abrocitinib (Cibinqo) in the integrated safety analysis, including the long term extension study, the rate of serious infections was 2.43 per 100 patient-years in the Abrocitinib (Cibinqo) 100 mg group and 2.46 per 100 patient-years in the Abrocitinib (Cibinqo) 200 mg group. The most commonly reported serious infections were herpes simplex, herpes zoster, and pneumonia (see Precautions).
Opportunistic infections: Most opportunistic infections were cases of multidermatomal cutaneous herpes zoster. Among all patients treated with Abrocitinib (Cibinqo), including the long-term extension study, the rate of opportunistic infections was 0.61 per 100 patient-years in the Abrocitinib (Cibinqo) 100 mg group and 1.23 per 100 patient-years in the Abrocitinib (Cibinqo) 200 mg group. Most cases of opportunistic herpes zoster were mild or moderate.
Thrombotic events including pulmonary embolism: Among all patients treated with Abrocitinib (Cibinqo) in the integrated safety analysis, including the long term extension study, the rate of PE was 0.08 per 100 patient-years in the Abrocitinib (Cibinqo) 100 mg group and, 0.17 per 100 patient-years in the Abrocitinib (Cibinqo) 200 mg group. The rate of DVT was 0 per 100 patient-years in the Abrocitinib (Cibinqo) 100 mg group and 0.11 per 100 patient-years Abrocitinib (Cibinqo) 200 mg group (see Precautions).
Thrombocytopenia: In placebo-controlled studies, for up to 16 weeks, treatment with Abrocitinib (Cibinqo) was associated with a dose-related decrease in platelet count. Maximum effects on platelets were observed within 4 weeks, after which the platelet count returned towards baseline despite continued therapy. Confirmed platelet counts of <50 × 103/mm3 were reported in 0.1% of patients exposed to Abrocitinib (Cibinqo) 200 mg, 0 patients treated with Abrocitinib (Cibinqo) 100 mg or placebo. Among all patients exposed to Abrocitinib (Cibinqo) in the integrated safety analysis, including the long term extension study, the rate of confirmed platelet counts of <50 × 103/mm3 was 0.17 per 100 patient-years for 200 mg and 0 per 100 patient-years for 100 mg, most occurring at Week 4. Patients 65 years of age and older had a higher rate of platelet counts <75 × 103/mm3 (see Precautions). There were no adolescent patients who developed platelet counts <75 × 103/mm3.
Lymphopenia: In placebo-controlled studies, for up to 16 weeks, confirmed ALC <0.5 × 103/mm3 occurred in 2 patients (0.3%) treated with Abrocitinib (Cibinqo) 200 mg and 0 patients treated with Abrocitinib (Cibinqo) 100 mg or placebo. Both cases occurred in the first 4 weeks of exposure. Among all patients exposed to Abrocitinib (Cibinqo) in the integrated safety analysis, including the long term extension, the rate of confirmed ALC <0.5 × 103/mm3 was 0.56 per 100 patient-years for 200 mg and 0 patient-years for 100 mg, the highest rate was observed in patients 65 years of age and older (see Precautions). There were no adolescent patients who developed an ALC <0.5 x 103/mm3.
Lipid elevations: In placebo controlled studies, for up to 16 weeks, there was a dose-related percent increase in low density lipoprotein cholesterol (LDL-c), total cholesterol, and high density lipoprotein cholesterol (HDL-c) relative to placebo at Week 4 which remained elevated through the final visit in the treatment period. The median % change in LDL-c at Week 4 was 9.1%, 4.9% and -2.8% in patients exposed to 200 mg, 100 mg and placebo, respectively. The median % change in HDL-c at Week 4 was 20.0%, 12.1%, and 0% in patients exposed to 200 mg, 100 mg and placebo, respectively. Events related to hyperlipidemia occurred in 0.4% of patients exposed to Abrocitinib (Cibinqo) 100 mg, 0.6% of patients exposed to 200 mg, and 0% of patients exposed to placebo (see Precautions).
Creatine phosphokinase elevations (CPK): In placebo-controlled studies, for up to 16 weeks, events of blood CPK increased (>5 × ULN) were reported in 3.8% of patients treated with 200 mg, 1.8% of patients treated with 100 mg of Abrocitinib (Cibinqo), and 1.8% of patients treated with placebo. Most elevations were transient, and none led to discontinuation.
Nausea: Nausea was most frequent in the first week of Abrocitinib (Cibinqo) therapy and generally resolved with continued therapy. The median duration of nausea was 15 days. Most of the cases were mild to moderate in severity.
Pediatric population: A total of 635 adolescent patients (12 to less than 18 years of age) were treated with Abrocitinib in clinical studies in atopic dermatitis representing 851.5 patient-years of exposure. The safety profile observed in adolescents in atopic dermatitis clinical studies was similar to that of the adult population.
View ADR Monitoring Form