Ciclosporin (Ikervis) is an ophthalmic emulsion containing 1 mg of Ciclosporin in each mL, or 0.3 mg of Ciclosporin in each single-dose container (0.3 mL). It also contains medium-chain triglycerides, cetalkonium chloride, glycerol, and tyloxapol, poloxamer 188, sodium hydroxide (to adjust pH) and water for injections.
Pharmacology: Pharmacodynamics: Clinical studies: Treatment of severe keratitis in dry eye disease: The efficacy and safety of Ciclosporin (Ikervis) were evaluated in two randomised, double-masked, vehicle-controlled clinical studies in adult patients with dry eye disease (keratoconjunctivitis sicca) who met the International Dry Eye Workshop (DEWS) criteria.
In the 12 month, double-masked, vehicle controlled, pivotal clinical trial (SANSIKA study), 246 Dry Eye Disease (DED) patients with severe keratitis (defined as a corneal fluorescein staining (CFS) score of 4 on the modified Oxford scale) were randomised to one drop of Ciclosporin (Ikervis) or vehicle daily at bedtime for 6 months. Patients randomised to the vehicle group were switched to Ciclosporin (Ikervis) after 6 months. The primary endpoint was the proportion of patients achieving by Month 6 at least a two-grade improvement in keratitis (CFS) and a 30% improvement in symptoms, measured with the Ocular Surface Disease Index (OSDI). The proportion of responders in the Ciclosporin (Ikervis) group was 28.6%, compared to 23.1% in the vehicle group. The difference was not statistically significant (p=0.326).
The severity of keratitis, assessed using CFS, improved significantly from baseline at Month 6 with Ciclosporin (Ikervis) compared to vehicle (mean change from baseline was -1.764 with Ciclosporin (Ikervis) vs. -1.418 with vehicle, p=0.037). The proportion of Ciclosporin (Ikervis)-treated patients with a 3-grade improvement in CFS score at Month 6 (from 4 to 1) was 28.8%, compared to 9.6% of vehicle-treated subjects, but this was a post-hoc analysis, which limits the robustness of this outcome. The beneficial effect on keratitis was maintained in the open phase of the study, from Month 6 and up to Month 12.
The mean change from baseline in the 100-point OSDI score was ‑13.6 with Ciclosporin (Ikervis) and ‑14.1 with vehicle at Month 6 (p=0.858). In addition, no improvement was observed for Ciclosporin (Ikervis) compared to vehicle at Month 6 for other secondary endpoints, including ocular discomfort score, Schirmer test, use of concomitant artificial tears, investigator's global evaluation of efficacy, tear break-up time, lissamine green staining, quality of life score, and tear osmolarity.
A reduction in the ocular surface inflammation assessed with Human Leukocyte Antigen-DR (HLA-DR) expression (an exploratory endpoint), was observed at Month 6 in favour of Ciclosporin (Ikervis) (p=0.021).
In the 6 month, double-masked, vehicle controlled, supportive clinical trial (SICCANOVE study), 492 DED patients with moderate to severe keratitis (defined as a CFS score of 2 to 4) were also randomised to Ciclosporin (Ikervis) or vehicle daily at bedtime for 6 months. The co-primary endpoints were the change in CFS score, and the change in global score of ocular discomfort unrelated to study medication instillation, both measured at Month 6. A small but statistically significant difference in CFS improvement was observed between the treatment groups at Month 6 in favour of Ciclosporin (Ikervis) (mean change from baseline in CFS -1.05 with Ciclosporin (Ikervis) and -0.82 with vehicle, p=0.009).
The mean change from baseline in ocular discomfort score (assessed using a Visual Analogic Scale) was -12.82 with Ciclosporin (Ikervis) and -11.21 with vehicle (p=0.808).
In both studies, no significant improvement of symptoms was observed for Ciclosporin (Ikervis) compared to vehicle after 6 months of treatment, whether using a visual analogue scale or the OSDI.
In both studies one third of the patients in average had Sjögren's syndrome; as for the overall population, a statistically significant improvement in CFS in favour of Ciclosporin (Ikervis) was observed in this subgroup of patients.
At completion of the SANSIKA study (12 month study), patients were asked to enter the Post SANSIKA study. This study was an open-label, non-randomized, one-arm, 24-month study extension of the Sansika Study. In Post SANSIKA study patients alternatively received Ciclosporin (Ikervis) treatment or no treatment depending on CFS score (patients received Ciclosporin (Ikervis) when there was a worsening of keratitis).
This study was designed to monitor the long-term efficacy and relapse rates in patients who have previously received Ciclosporin (Ikervis).
The primary objective of the study was to assess the duration of the improvement following Ciclosporin (Ikervis) treatment discontinuation once the patient was improved with respect to the baseline of the SANSIKA study (i.e. at least 2 grade improvement on the modified Oxford scale).
67 patients were enrolled (37.9% of the 177 patients having ended SANSIKA). After the 24-month period, 61.3% of 62 patients included in the primary efficacy population did not experience a relapse based on CFS scores. Percentage of patients who experienced a severe keratitis recurrence was 35% and 48% in patients treated 12 months and 6 months with Ciclosporin (Ikervis) respectively in the SANSIKA study.
Based on the first quartile (the median could not be estimated due to the small number of relapses), time to relapse (back to CFS grade 4) was ≤224 days and ≤175 days in patients previously treated 12 months and 6 months with Ciclosporin (Ikervis), respectively. Patients spent more time on CFS grade 2 (Median 12.7 weeks/year) and grade 1 (Median 6.6 weeks/year) than CFS grade 3 (Median 2.4 weeks/year), CFS grades 4 and 5 (Median time 0 week/year).
Assessment of DED symptoms by VAS showed a worsening of patient's discomfort from the time treatment was first stopped to the time it was restarted except pain which remained relatively low and stable. The median global VAS score increased from the time treatment was first stopped (23.3%) to the time treatment was restarted (45.1%).
No significant changes have been observed in the other secondary endpoints (TBUT, lissamine green staining and Schirmer test, NEI-VFQ and EQ-5D) over the course of the extension study.
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Ciclosporin (Ikervis) in all subsets of the paediatric population for dry eye disease (see Dosage & Administration for information on paediatric use).
Treatment of severe vernal keratoconjunctivitis (VKC): In a 12 month double-masked, vehicle controlled, pivotal clinical trial (VEKTIS study), 169 patients with severe VKC and severe keratitis (grade 4 or 5 on the modified Oxford scale) were randomised to 4 drops (high dose) or 2 drops (low dose) of ciclosporin 1 mg/mL eye drops emulsion and 2 drops or 4 drops of vehicle for the first 4 months (Period 1). Patients randomised to the vehicle group were switched to ciclosporin 1 mg/mL eye drops emulsion (four times or twice daily) from Month 4 to Month 12 (Period 2).
168 patients [127 children (75.6%) and 41 adolescents (24.4%)] were included in the efficacy analyses. Mean age was 9.2 years (SD: 3.3, age range: 4-17 years). There were more male [n=132 (78.6%)] than female patients [n=36 (21.4%)].
The primary efficacy endpoint which was the average penalties adjusted change of the Corneal Fluorescein Staining (CFS) score from baseline and over Period 1, considered all patients (n=168). Efficacy was assessed every month during the 4 month treatment period and compared with baseline using a composite criterion based on keratitis assessed by the modified Oxford scale, the need for rescue medicinal product (use of topical steroids) and the occurrence of corneal ulceration.
The difference in the Least Square (LS) mean vs. vehicle was 0.76 (95% CI: 0.26, 1.27) for the high dose group and 0.67 (95% CI: 0.16, 1.18) for the low dose group. Both differences were statistically significant with p=0.007 for the high dose and p=0.010 for the low dose group.
Clinical relevance of the primary efficacy endpoint was however difficult to address. In that context, responder rate's results were considered as more reliable endpoint. A responder was defined as a patient 1) with a mean CFS score over the 4 months of treatment ≤ 50% of baseline, 2) who did not withdraw from the study for a reason possibly due to treatment, 3) with no experience of corneal ulceration and 4) no use of rescue medicinal product in the last 4 months of treatment. There was a significantly higher number of CFS responders in both active groups as compared to vehicle (p=0.005 for the high dose group, and p=0.010 for the low dose group) with 55.4%, 50.0% and 27.6% of responders in the high dose, low dose and vehicle groups respectively. The excess rate with respect to vehicle was 27.8% for the high dose regimen and 22.4% for the low dose one.
Rescue medicinal product (topical steroids) was used more often in the vehicle than in the high dose regimen: 32.1% in the high dose group and 31.5% in the low dose group received at least one course of rescue medicinal product while they were 53.4% in the vehicle group.
All four symptoms (photophobia, tearing, itching and mucous discharge) improved over time and the difference from baseline at Month 4 for each symptom largely exceeded 10 mm.
For the average of VKC symptoms, the difference in the LS mean vs. vehicle in the high dose group was statistically significant at all time points compared to vehicle: -19.4 mm (p<0.05).
Patient quality of life (Quick questionnaire) improved significantly better in the high dose group compared to vehicle. The improvement was clinically relevant as illustrated by the effect size over 4 months (symptoms domain: 0.67 and daily activities domain: 0.44).
In Period 2, analyses demonstrated stability of improvements achieved during Period 1 for both doses regimen.
Treatment of severe keratitis in dry eye disease: Treatment of severe keratitis in adult patients with dry eye disease, which has not improved despite treatment with tear substitutes.
Treatment of severe vernal keratoconjunctivitis (VKC): Treatment of severe vernal keratoconjunctivitis (VKC) in children and adolescents from 4 to 18 years old.
Ciclosporin (Ikervis) treatment must be initiated by an ophthalmologist or a healthcare professional qualified in ophthalmology.
Dosage: Treatment of severe keratitis in dry eye disease: Adults: The recommended dose is one drop of Ciclosporin (Ikervis) once daily to be applied to the affected eye(s) at bedtime.
Response to treatment should be reassessed at least every 6 months.
If a dose is missed, treatment should be continued on the next day as normal. Patients should be advised not to instill more than one drop in the affected eye(s).
Elderly patients: The elderly population has been studied in clinical studies. No dose adjustment is required.
Patients with renal or hepatic impairment: The effect of Ciclosporin (Ikervis) has not been studied in patients with hepatic or renal impairment.
However, no special considerations are needed in these populations.
Paediatric population: There is no relevant use of Ciclosporin (Ikervis) treatment of severe keratitis in adult patients with dry eye disease, which has not improved despite treatment with tear substitutes.
Treatment of severe VKC: Children from 4 years of age and adolescents: The recommended dose is one drop of Ciclosporin (Ikervis) 4 times a day (morning, noon, afternoon and evening) to be applied to each affected eye during the VKC season. If signs and symptoms of VKC persist after the end of the season, the treatment can be maintained at the recommended dose or decreased to one drop twice daily once adequate control of signs and symptoms is achieved. Treatment should be discontinued after signs and symptoms are resolved, and reinitiated upon their recurrence.
Efficacy and safety of IKERVIS in VKC has not been studied beyond 12 months. (see Precautions).
If a dose is missed, treatment should be continued on the next instillation as normal. Patients should be advised not to instill more than one drop for each instillation in the affected eye(s).
Children below 4 years: There is no relevant use of Ciclosporin (Ikervis) in the treatment of VKC in children below 4 years.
Adults: The effect of Ciclosporin (Ikervis) in VKC has not been studied in patients above 18 years of age.
Patients with renal or hepatic impairment: The effect of Ciclosporin (Ikervis) in VKC has not been studied in patients with renal or hepatic impairment. However, no special dose adjustment is needed in these populations.
Administration: Ocular use.
Precautions to be taken before administering the medicinal product: Patients should be instructed to first wash their hands.
Prior to administration, the single-dose container should be gently shaken.
For single use only. Each single-dose container is sufficient to treat both eyes. Any unused emulsion should be discarded immediately. Patients should be instructed to use nasolacrimal occlusion and to close the eyelids for 2 minutes after instillation, to reduce the systemic absorption. This may result in a decrease in systemic undesirable effects and an increase in local activity (see Precautions).
If more than one topical ophthalmic medicinal product is being used, the medicinal products must be administered at least 15 minutes apart. Ciclosporin (Ikervis) should be administered last (see Precautions).
A topical overdose is not likely to occur after ocular administration. If overdose with Ciclosporin (Ikervis) occurs, treatment should be symptomatic and supportive.
Hypersensitivity to the active substance or to any of the excipients.
Active or suspected ocular or peri-ocular infection.
Patients with ocular malignancies or premalignant conditions.
Treatment of severe keratitis in dry eye disease: Ciclosporin (Ikervis) has not been studied in patients with a history of ocular herpes and should therefore be used with caution in such patients.
Contact lenses: Patients wearing contact lenses have not been studied. Careful monitoring of patients with severe keratitis is recommended. Contact lenses should be removed before instillation of the eye drops at bedtime and may be reinserted at wake-up time.
Concomitant therapy: There is limited experience with Ciclosporin (Ikervis) in the treatment of patients with glaucoma. Caution should be exercised when treating these patients concomitantly with Ciclosporin (Ikervis), especially with beta-blockers which are known to decrease tear secretion.
Effects on the immune system: Medicinal products, which affect the immune system, including ciclosporin, may affect host defences against infections and malignancies.
Co-administration of Ciclosporin (Ikervis) with eye drops containing corticosteroids could potentiate the effects of Ciclosporin (Ikervis) on the immune system (see Interactions).
Treatment of severe VKC: Ciclosporin (Ikervis) has not been studied in patients with an active orofacial herpes simplex infection, a history of ocular herpes, varicella-zoster, or vaccinia virus infection and should therefore be used with caution in such patients.
Contact lenses: Patients wearing contact lenses have not been studied. Therefore, the use of Ciclosporin (Ikervis) with contact lenses is not recommended.
Concomitant therapy: Co-administration of Ciclosporin (Ikervis) with eye drops containing corticosteroids may potentiate the effects of Ciclosporin (Ikervis) on the immune system. However, in clinical studies, 18 patients received 4 times daily doses with co-administration of eye drops containing corticosteroids and no increase in the risk of adverse reactions related to the immune system was identified. Therefore, caution should be exercised when corticosteroids are administered concomitantly with Ciclosporin (Ikervis). (See Interactions.)
Effects on the immune system: Ophthalmic medicinal products, which affect the immune system, including ciclosporin, may affect host defenses against local infections and malignancies. Therefore, regular examination of the eye(s) is recommended, e.g. every 3 to 6 months, when Ciclosporin (Ikervis) is used for more than 12 months.
Treatment duration: Efficacy and safety of Ciclosporin (Ikervis) have not been studied beyond 12 months. Therefore, regular examination of the eye(s) is recommended, e.g. every 3 to 6 months, when used for more than 12 months.
Excipient: Ciclosporin (Ikervis) contains cetalkonium chloride which may cause eye irritation.
Effects on ability to drive and use machines: Ciclosporin (Ikervis) has moderate influence on the ability to drive and use machines.
This medicinal product may induce temporary blurred vision or other visual disturbances which may affect the ability to drive or use machines (see Adverse Reactions). Patients should be advised not to drive or use machines until their vision has cleared.
Women of childbearing potential/contraception in females: Ciclosporin (Ikervis) is not recommended in women of childbearing potential not using effective contraception.
Pregnancy: There is no data from the use of Ciclosporin (Ikervis) in pregnant women.
Studies in animals have shown reproductive toxicity following systemic administration of Ciclosporin at exposure considered sufficiently in excess of the maximum human exposure indicating little relevance to the clinical use of Ciclosporin (Ikervis).
Ciclosporin (Ikervis) is not recommended during pregnancy unless the potential benefit to the mother outweighs the potential risk to the fetus.
Breast-feeding: Following oral administration, Ciclosporin is excreted in breast milk. There is insufficient information on the effects of Ciclosporin in newborns/infants. However, at therapeutic doses of Ciclosporin in eye drops, it is unlikely that sufficient amounts would be present in breast milk. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from Ciclosporin (Ikervis) therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman.
Fertility: There is no data on the effects of Ciclosporin (Ikervis) on human fertility.
No impairment of fertility has been reported in animals receiving intravenous Ciclosporin.
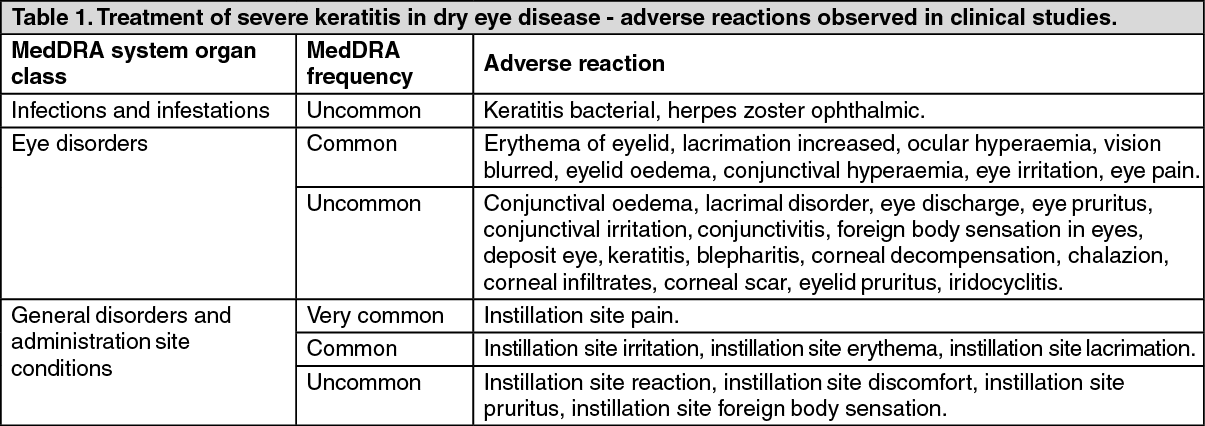
Summary of the safety profile: Tabulated list of adverse reactions: Adverse reactions listed in Tables 1 and 2 as follows were observed in clinical studies. They are ranked according to system organ class and classified according to the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), or not known (cannot be estimated from the available data).
Treatment of severe keratitis in dry eye disease: In five clinical studies including 532 patients who received Ciclosporin (Ikervis) and 398 who received Ciclosporin (Ikervis) vehicle (control), Ciclosporin (Ikervis) was administered at least once a day in both eyes, for up to one year. The most common adverse reactions were eye pain (19.2%), eye irritation (17.8%), lacrimation (6.4%), ocular hyperaemia (5.5%) and eyelid erythema (1.7%) which were usually transitory and occurred during instillation.
The majority of adverse reactions reported in clinical studies with the use of Ciclosporin (Ikervis) were ocular and mild to moderate in severity. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Treatment of severe VKC: The most common adverse reactions in the clinical trials were eye pain (11%) and eye pruritus (9%) which were usually transitory and occurred during instillation. (See Table 2.)
Click on icon to see table/diagram/image
Description of selected adverse reactions: Instillation site pain was a frequently reported local adverse reaction associated with the use of Ciclosporin (Ikervis) during clinical trials. It is likely to be attributable to ciclosporin.
One case of severe epithelial erosion of the cornea identified as corneal decompensation by the investigator resolved without sequelae was reported.
Patients receiving immunosuppressive therapies, including ciclosporin, are at increased risk of infections. Both generalised and localised infections can occur. Pre-existing infections may also be aggravated (see Contraindications). Cases of infections have been reported uncommonly in association with the use of Ciclosporin (Ikervis). To reduce the systemic absorption, see Dosage & Administration.
No interaction studies have been performed with Ciclosporin (Ikervis).
Combination with other medicinal products that affect the immune system: Co-administration of Ciclosporin (Ikervis) with eye drops containing corticosteroids could potentiate the effects of Ciclosporin on the immune system (see Precautions).
Severe VKC: In clinical studies, 18 patients received Ciclosporin (Ikervis) 4 times daily in co-administration with eye drops containing corticosteroids and no increase of the risk of adverse reactions related to the immune system were identified (see Precautions).
Do not freeze.
Store below 30°C.
Keep single-dose containers in the pouch in order to protect from light and avoid evaporation.
Discard the opened single-dose container immediately after use.
S01XA18 - ciclosporin ; Belongs to the class of other ophthalmologicals .
Ikervis ophth emulsion 1 mg/mL
0.3 mL x 30 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image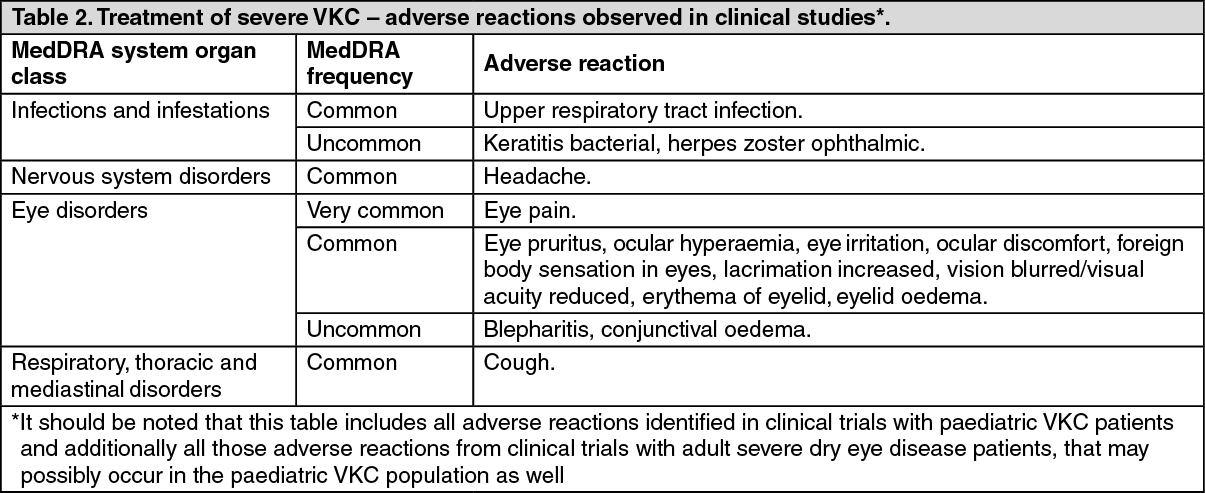 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out