1 prolonged release tablet contains 5 mg felodipine and 47.5 mg metoprolol succinate equivalent to 50 mg metoprolol tartrate.
Felodipine/Metoprolol succinate (LOGIMAX) prolonged release tablets contain metoprolol succinate in the form of granules, which each form an individual depot unit, and which together with felodipine are embedded in a polymer. In contact with fluid a gel layer is formed, which permits continuous release of both felodipine and metoprolol.
Pharmacotherapeutic group: Calcium antagonists and β-blockers. ATC code: C07FB02.
Pharmacology: Pharmacodynamics: Felodipine/Metoprolol succinate (LOGIMAX) is an antihypertensive preparation consisting of a combination of felodipine, which is a calcium antagonist with a selective effect on pre-capillary resistance vessels, and metoprolol, which is a β1-selective receptor blocker.
As a result of the mechanisms of action of the two substances complementing each other (felodipine reduces peripheral vascular resistance and metoprolol reduces cardiac output), a more pronounced antihypertensive effect is obtained than with either of the two drugs in monotherapy. With Felodipine/Metoprolol succinate (LOGIMAX) an even and effective lowering of blood pressure over the entire interval between doses (24 hours) is achieved.
Felodipine: Felodipine is a vascular selective calcium antagonist for the treatment of hypertension and stable angina pectoris. Felodipine is a dihydropyridine derivative and a racemate.
Felodipine acts by reducing peripheral vascular resistance, especially in arterioles. The electrical and contractile activity in the smooth muscle cells in the vessels is inhibited via an effect on the calcium channels in the cell membrane.
As a result of felodipine having a selective effect on smooth muscle in the arterioles, in therapeutic doses it has no negative inotropic effect on the heart and no clinically significant electrophysiological effect in the heart. Felodipine relaxes smooth muscle in the respiratory tract. Clinical experience has shown that felodipine has little effect on gastrointestinal motoricity. No clinically significant effect of felodipine on blood lipid values has been observed during long-term treatment. Nor has any clinically significant effect on metabolic control (HbA1c) been observed in patients with type II diabetes during 6 months of treatment.
Felodipine can generally also be given to patients who also have reduced left ventricular function who are being treated with the usual therapy, and to those who have asthma, diabetes, gout or hyperlipidemia.
Antihypertensive effect: Felodipine lowers arterial blood pressure by reducing peripheral vascular resistance. Treatment of hypertensive patients with felodipine produces a lowering of blood pressure in supine, seated and standing position, at rest and during exercise. Felodipine does not cause orthostatic hypotension, as the substance does not affect smooth muscle in the veins or adrenergic control mechanisms. The lowered blood pressure may initially result in a transient, reflectory increase in heart rate and cardiac output. The increase in heart rate is counteracted if felodipine is given in combination with β-blockers. The effect on blood pressure and total peripheral vascular resistance is correlated to the plasma concentration of felodipine. In steady state the effect lasts for the entire interval between doses, and produces a lowering of blood pressure for the whole day.
Treatment with felodipine produces a regression of left ventricular hypertrophy.
Felodipine has a natriuretic and diuretic but no kaliuretic effect. Tubular reabsorption of sodium and water is reduced, which may explain the absence of salt and fluid retention in patients. Felodipine reduces renal vascular resistance and increases renal perfusion. Glomerular filtration is not affected. Felodipine does not affect albumin excretion.
Metoprolol: Metoprolol is a β1-selective receptor blocker, which means that metoprolol influences the cardiac β1-receptors in lower doses than those required to influence β2-receptors in peripheral vessels and bronchi.
Metoprolol is devoid of a β-stimulant effect and has little membrane-stimulating effect. β-receptor blockers have negative inotropic and chronotropic effects.
Treatment with metoprolol reduces the effect of catecholamines connected with physical and psychological stress and produces a lower heart rate, lower cardiac output and lower blood pressure. In stress states with increased secretion of adrenaline from the adrenals, metoprolol does not prevent the normal physiological vasodilatation. In therapeutic doses, metoprolol has less contractile effect on the bronchial musculature than non-selective β-blockers. This property makes it possible to treat patients with bronchial asthma or other pronounced obstructive pulmonary disease with metoprolol in combination with β2-receptor stimulants. Metoprolol influences insulin secretion and carbohydrate metabolism to a lesser degree than non-selective β-blockers, and can therefore also be given to patients with diabetes mellitus. The cardiovascular reaction in hypoglycemia, e.g. tachycardia, is affected to a lesser degree by metoprolol, and the return of the blood sugar level to normal takes place more rapidly than with non-selective β-receptor blockers.
In hypertension metoprolol produces a marked lowering of blood pressure in both supine and standing position and during physical effort. Initially, treatment with metoprolol causes an increase in peripheral vascular resistance. During long-term treatment, however, the achieved lowering of blood pressure is attributed to reduced peripheral vascular resistance and an unchanged cardiac output. Metoprolol reduces the risk of cardiovascular death in men with moderate/severe hypertension. Disturbances of electrolyte balance do not occur.
Pharmacokinetics: Felodipine: Bioavailability is approx. 15% and is not influenced by concomitant food intake. The rate of absorption - but not the degree of absorption - is affected by concomitant food intake, which is why the maximum plasma concentration increases by approx. 65%. The peak plasma concentration is reached after 3-5 hours. Binding to plasma proteins is approximately 99%. The volume of distribution in steady state is 10 L/kg. The half-life of felodipine in the elimination phase is approx. 25 hours, and steady state is reached after 5 days. There is no risk of accumulation during long-term treatment. Clearance is on average 1200 mL/min. Reduced clearance in elderly patients and patients with impaired hepatic function leads to these having higher plasma concentrations of felodipine. However, age only partially explains the inter-individual variations in plasma concentration. Felodipine is metabolized in the liver, and all identified metabolites are devoid of vasodilator effects. Approx. 70% of a given dose is excreted as metabolites via the urine, the remainder in the feces. Less than 0.5 % of a given dose is excreted in unchanged form in the urine. Impaired renal function does not affect the plasma concentration of felodipine, but accumulation of inactive metabolites occurs. Felodipine is not eliminated by hemodialysis.
Metoprolol: Absorption after oral administration is complete, and the substance is absorbed along the entire gastrointestinal tract, also in the colon. The bioavailability of Metoprolol Succinate (Betazok) is 30-40%. Metoprolol is metabolized in the liver mainly by CYP2D6. Three main metabolites have been identified, but none with a β-blocking effect of clinical significance. Approx. 5% of metoprolol is excreted via the kidneys in unchanged form, the remainder of the dose in the form of metabolites.
Characteristics of combination products: On administration of Felodipine/Metoprolol succinate (LOGIMAX) the bioavailability of neither metoprolol nor felodipine is altered, compared with concomitant administration of metoprolol and felodipine. Absorption is not influenced by concomitant intake of food.
Toxicology: Preclinical safety data: Available studies concerning general toxicity, genotoxicity and carcinogenicity did not reveal any special risks for humans. In animal studies β-receptor blockers caused bradycardia in the fetuses. In several species calcium antagonists have caused embryotoxic and/or teratogenic effects, mainly in the form of distal skeletal malformations. In reproduction toxicology studies with felodipine, prolonged pregnancy and difficult parturition were observed in rats, and in rabbits poorer development of distal phalanges was seen (probably caused by reduced uteroplacental perfusion). These observations do not indicate direct teratogenic effects, but suggest secondary consequences of the pharmacodynamic effects of felodipine.
Hypertension. Felodipine/Metoprolol succinate (LOGIMAX) can be used when treatment with β-blockers or calcium antagonists of the dihydropyridine type in monotherapy has not produced an adequate effect.
The dosage is individual. The starting dose is based on experience from earlier treatment with β-receptor blockers or calcium antagonists. The normal dosage is one Felodipine/Metoprolol succinate (LOGIMAX) prolonged release tablet (5 mg/47.5 mg) per day. If required, the dose may be increased to twice daily.
The prolonged release tablet is given once daily, in the morning. The prolonged release tablet must be swallowed with water, and must not be divided, crushed or chewed. The prolonged release tablet may be taken on an empty stomach or together with a light meal with a low fat and carbohydrate content.
Impaired renal function: Impaired renal function does not affect the plasma concentration. No dose adjustment is required. However, Felodipine/Metoprolol succinate (LOGIMAX) must be used with caution in patients with severely impaired renal function. (See Precautions and Pharmacology: Pharmacokinetics under Actions.)
Impaired hepatic function: A dose adjustment is not usually necessary for patients with hepatic cirrhosis since metoprolol has a low degree of protein binding (5-10%). If there are signs of very severely impaired hepatic function (e.g. patients who have undergone shunt surgery) doses higher than Felodipine/Metoprolol succinate (LOGIMAX) (5 mg/ 47.5 mg) must not be given.
Elderly patients: One Felodipine/Metoprolol succinate (LOGIMAX) prolonged release tablet per day is usually sufficient. If required, the dose may be increased to twice daily.
Children: There is a lack of experience of treatment of children.
Toxicity: Felodipine: 10 mg in a 2-year-old caused mild intoxication. 150-200 mg in a 17-year-old and 250 mg in an adult caused mild to moderate intoxication. Probably a more pronounced effect on the peripheral circulation than on the heart, compared with other drugs in the group.
Metoprolol: 7.5 g in an adult caused fatal intoxication. 100 mg in a 5-year-old caused no symptoms after gastric lavage. 450 mg in a 12-year-old and 1.4 g in an adult caused moderate intoxication, 2.5 g in an adult caused severe intoxication, 7.5 g in an adult caused very severe intoxication.
Symptoms: In cases of intoxication with prolonged release preparations the onset of symptoms may be delayed for 12-16 hours, and severe symptoms may occur after several days.
Felodipine: The effect on the circulation constitutes the greatest risk: bradycardia (sometimes tachycardia), fall in blood pressure. AV block I-III, AV dissociation, VES, ventricular fibrillation, asystole. Dizziness, headache, impaired consciousness, coma, convulsions. Dyspnea, pulmonary edema (non-cardiac) and apnea. Possibly ARDS (Adult Respiratory Distress Syndrome). Acidosis, hypokalemia, hyperglycemia, possibly hypocalcemia. Flushing, hypothermia. Nausea and vomiting.
Metoprolol: Cardiovascular symptoms the most important, but in some cases, especially in children and adolescents, CNS symptoms and respiratory depression may predominate. Bradycardia. AV block I-III, asystole, fall in blood pressure, poor peripheral blood perfusion, cardiac incompensation, cardiogenic shock. Respiratory depression, apnea. Other: Fatigue, muzziness, unconsciousness, fine tremor, convulsions, sweating, paresthesia, bronchospasm, nausea, vomiting, possibly esophageal spasm, hypoglycemia (especially in children), or hyperglycemia, hyperkalemia. Effect on the kidneys. Transient myasthenic syndrome. Concomitant ingestion of alcohol, antihypertensive drugs, quinidine or barbiturates can aggravate the patient's condition. The first signs of overdose may be seen 20 minutes to 2 hours after ingestion.
Treatment: Felodipine: Charcoal, if necessary gastric lavage, in some cases even at a late stage. NOTE! Atropine (0.25-0.5 mg intravenously for adults, 10-20 micrograms/kg for children) should be given before gastric lavage (on account of the risk of vagal stimulation). ECG monitoring. Respirator treatment if indicated. Correction of acid-base and electrolyte status. In cases of bradycardia and block: Atropine 0.5-1 mg intravenously for adults (20-50 micrograms/kg for children), possibly repeated, or isoprenaline initially 0.05-0.1 micrograms/kg/minute. Pacemaker at an early stage in severe cases. In cases of hypotension: intravenous fluid, calcium glubionate (9 mg Ca/mL) 20(-30) mL intravenously over a period of 5 minutes for adults (3-5 mg Ca/kg for children) initially and repeated if required, or as an infusion, adrenaline or dopamine if required. In severe cases glucagon may be tried. In cases of circulatory arrest in connection with overdose, attempts at resuscitation for several hours may be necessary. Diazepam for convulsions. Other symptomatic treatment.
Metoprolol: Charcoal, gastric lavage if required. NOTE! Atropine (0.25-0.5 mg intravenously for adults, 10-20 micrograms/kg for children) should be given before gastric lavage (on account of the risk of vagal stimulation). Intubation and respirator treatment should be carried out if indicated. Adequate volume expansion. Glucose infusion. ECG monitoring. Atropine 1.0-2.0 mg intravenously, possibly repeated (especially in cases of vagal symptoms). For myocardial depression: infusion of dobutamine or dopamine and calcium glubionate 9 mg/mL, 10-20 mL. Glucagon 50-150 micrograms/kg intravenously over a period of 1 minute followed by infusion may also be tried, as can amrinone. In some cases the addition of epinephrine (adrenaline) has been effective. Infusion of sodium (chloride or bicarbonate) in cases of widening QRS-complex and arrhythmias. Possibly pacemaker. In cases of circulatory arrest in connection with overdose resuscitation measures for several hours may be necessary. For bronchospasm possibly terbutaline (via injection or inhalation). Symptomatic therapy
Known hypersensitivity to any of the components of the product or to other dihydropyridines or β-blockers. Pregnancy. Unstable angina pectoris. Degree II and III AV block. Patients with unstable uncompensated heart failure (pulmonary edema, hypoperfusion or hypotension), and patients with continuous or intermittent inotropic therapy with β-receptor agonism. Symptomatic bradycardia or hypotension. Sick sinus syndrome. Cardiogenic shock. Severe peripheral vascular disease with threat of gangrene. Felodipine/Metoprolol succinate (LOGIMAX) must not be given to patients with suspected acute myocardial infarction with a heart rate of <45 beats/minute, P Q interval >0.24 seconds or systolic blood pressure <100 mmHg.
Combination treatment with digitalis. Felodipine/Metoprolol succinate (LOGIMAX) can exacerbate the symptoms of peripheral vascular disease, e.g. intermittent claudication. Severely impaired renal function (GFR <30 mL/min). Aortic stenosis. Impaired hepatic function. Heart failure following acute myocardial infarction. Acute myocardial infarction. Hypotension, which in susceptible subjects can cause myocardial ischemia. Severe acute pathological conditions with metabolic acidosis.
Felodipine/Metoprolol succinate (LOGIMAX) must not be used for first treatment of previously untreated patients.
Felodipine/Metoprolol succinate (LOGIMAX) should not be given to patients with latent or manifest cardiac insufficiency without concomitant treatment of this.
Treatment with Felodipine/Metoprolol succinate (LOGIMAX) may affect carbohydrate metabolism or mask hypoglycemia, but the risk is less than with non-selective β-receptor blockers.
In isolated cases an existing moderate disturbance of AV-conduction time may be exacerbated (possibly leading to AV block).
Intravenous administration of verapamil must not be given to patients being treated with Felodipine/Metoprolol succinate (LOGIMAX).
In patients with Prinzmetal's angina the number and severity of angina attacks may increase, due to α-receptor-mediated constriction of coronary vessels. Non-selective β-blockers therefore must not be used for these patients. β1-selective receptor blockers must be used with care.
In cases of bronchial asthma or other chronic obstructive pulmonary diseases adequate bronchodilator therapy must be given concomitantly. The dose of β2-stimulants may need to be increased.
Treatment with β-blockers may make the treatment of an anaphylactic reaction more difficult. Adrenaline treatment in normal doses does not always produce the expected therapeutic effect.
If Felodipine/Metoprolol succinate (LOGIMAX) is given to patients with pheochromocytoma, treatment with α-blockers should be considered.
Concomitant administration of drugs that induce CYP3A4 leads to greatly reduced levels of felodipine and the risk of a lack of effect (see Interactions). This combination should be avoided.
Concomitant administration of drugs that are potent inhibitors of CYP3A4 leads to greatly increased levels of felodipine (see Interactions). This combination should be avoided. Concomitant ingestion of grapefruit juice leads to greatly increased levels of felodipine (see Interactions). This combination should be avoided. Concomitant ingestion of grapefruit juice leads to greatly increased levels of felodipine (see Interactions). This combination should be avoided.
Abrupt discontinuation of β-blockade, especially in high-risk patients, can be risky and can exacerbate chronic heart failure and increase the risk of myocardial infarction and sudden death. If possible, any discontinuation of Felodipine/Metoprolol succinate (LOGIMAX) should therefore take place gradually over a period of 1-2 weeks.
Prior to surgery, the anesthetist must be informed that the patient is on Felodipine/Metoprolol succinate (LOGIMAX). It is recommended that β-blocker treatment is not withdrawn in patients who are undergoing surgery.
Effects on ability to drive and use machines: Since dizziness and fatigue can occur during treatment with Felodipine/Metoprolol succinate (LOGIMAX), this should be taken into account when increased alertness is required, e.g. when driving or using machines.
Pregnancy: Felodipine/Metoprolol succinate (LOGIMAX) must not be given during pregnancy.
There is a lack of adequate data on treatment of pregnant women with felodipine. Felodipine must not be used during pregnancy, as fetal damage was seen in animal studies (see Pharmacology: Toxicology: Preclinical safety data under Actions). Calcium antagonists can inhibit premature contractions in the uterus, but definite confirmation of labor being prolonged in the case of a full-term pregnancy is lacking. A risk of fetal hypoxia may occur in the event of hypotension in the mother and reduced perfusion of the uterus on account of redistribution of the blood supply as a result of peripheral vasodilatation.
Metoprolol should be given during pregnancy and lactation only if it is absolutely necessary. β-receptor blockers can cause bradycardia in the fetus and new-born, and in the breast-fed infant. During the last trimester and in connection with parturition, therefore, the previously mentioned should be borne in mind when prescribing this preparation.
Lactation: Felodipine and metoprolol pass into breast milk. If the nursing mother takes therapeutic doses of felodipine, only a very small dose is transmitted to the infant via the breast milk. There is insufficient experience of felodipine treatment during lactation to permit an assessment of the risks for the infant. Felodipine is therefore not recommended during lactation. In cases in which the medical benefit of continued treatment is considered to predominate, the alternative of discontinuing breast-feeding should be considered.
The most common undesirable effects that were reported in clinical trials with Felodipine/Metoprolol succinate (LOGIMAX) are headache (11%), swelling of the ankles and facial redness. They may occur at the beginning of treatment or if the dose is increased, and are usually transient. Most of the undesirable effects are due to the vasodilator properties of felodipine. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For felodipine the following undesirable effects have also been reported: (See Table 2).
Click on icon to see table/diagram/image
Isolated cases of confusion of sleep disturbance have been reported, but a connection with felodipine could not definitely be established.
Cases of gingival hyperplasia have been described after treatment with felodipine in patients with pronounced gingivitis/parodontitis. The swelling may be avoided or reduced by means of careful oral hygiene. Hyperglycemia is considered to be a group-specific adverse reaction, but for felodipine has been reported only in isolated cases.
For metoprolol the following undesirable effects have also been reported: (See Table 3).
Click on icon to see table/diagram/image
Isolated cases of arthralgia, hepatitis, muscle cramps, dry mouth, conjunctivitis-like symptoms, rhinitis, impaired concentrations, and gangrene in patients with severe peripheral vascular disease have been reported.
Concomitant administration of substances that influence the cytochrome P450 system can affect the plasma concentration of both felodipine and metoprolol. Felodipine and metoprolol do not interact with each other, since they utilize different isoenzymes of cytochrome P450.
Interactions with felodipine: Felodipine is a CYP3A4 substrate. Drugs that inhibit or induce CYP3A4 greatly affect the plasma concentration of felodipine.
Cytochrome P450 inducers: Drugs that increase the metabolism of felodipine through induction of cytochrome P450 are e.g. carbamazepine, phenytoin, phenobarbital and rifampicin, and also St. John's wort (Hypericum perforatum). In cases of concomitant administration of carbamazepine, phenytoin and phenobarbital the felodipine AUC fell by 93% and the Cmax by 82%. Combination with CYP3A4 inducers should be avoided.
Cytochrome P450 inhibitors: Drugs that are potent CYP3A4 inhibitors are e.g. azole antifungal agents, (itraconazole, ketoconazole), macrolide antibiotics (erythromycin) and HIV-protease inhibitors. During concomitant administration of itraconazole, the felodipine Cmax increased 8-fold and the AUC 6-fold. During concomitant administration of erythromycin, the felodipine Cmax and AUC increased approximately 2.5-fold. Combination with potent CYP3A4 inhibitors should be avoided.
Grapefruit juice inhibits CYP3A4. Administration of felodipine in combination with grapefruit juice increased the felodipine Cmax and AUC approximately 2-fold. Combination with grapefruit juice should be avoided.
Tacrolimus: Felodipine can cause increased concentrations of tacrolimus. In cases of concomitant use, the serum concentration of tacrolimus must be monitored, and the tacrolimus dose may need to be adjusted.
Cyclosporin: During concomitant treatment with cyclosporin and felodipine the Cmax of felodipine increased by 150% and the AUC by approx. 60%. In contrast, the effect of felodipine on the kinetics of cyclosporin is marginal.
Cimetidine: During concomitant treatment with cimetidine and felodipine the Cmax and AUC of felodipine were increased by approx. 55%.
Interactions with metoprolol: Metoprolol is a CYP2D6-substrate. Drugs that inhibit CYP2D6 can have an effect on the plasma concentration of metoprolol. Examples of drugs that inhibit CYP2D6 are quinidine, terbinafine, paroxetine, fluoxetine, sertraline, celecoxib, propafenone and diphenhydramine. When treatment with these drugs are initiated the dose of Felodipine/Metoprolol succinate (LOGIMAX) might have to be reduced for patients treated with Felodipine/Metoprolol succinate (LOGIMAX).
The following combinations with Felodipine/Metoprolol succinate (LOGIMAX) should be avoided: Barbituric acid derivatives: Barbiturates (studied for pentobarbital) induce the metabolism of metoprolol to a slight degree through enzyme induction.
Propafenone: When propafenone was started in four patients who were already receiving treatment with metoprolol, the plasma concentrations of metoprolol increased 2-5-fold, and two patients experienced typical metoprolol side effects. The interaction was confirmed in tests on eight healthy trial subjects. The interaction is probably due to the fact that propafenone, like quinidine, inhibits the metabolism of metoprolol via cytochrome P4502D6. The combination is thought to be difficult to manage since propafenone also has β-receptor-blocking properties.
Verapamil: In combination with β-receptor blockers (has been described for atenolol, propranolol and pindolol), verapamil can cause bradycardia and a fall in blood pressure. Verapamil and β-blockers have additive inhibitory effects on AV conduction and sinus node function.
The following combinations with Felodipine/Metoprolol succinate (LOGIMAX) may require a dose adjustment: Class I antiarrhythmic drugs: Class I antiarrhythmic drugs and β-receptor blockers have additive negative inotropic effects, which can result in serious hemodynamic side effects in patients with impaired left ventricular function. The combination should also be avoided in "sick sinus syndrome" and pathological AV conduction. The interaction is best documented for disopyramide.
Diphenhydramine: Diphenhydramine reduces (2.5-fold) clearance of metoprolol to alpha-hydroxymetoprolol in rapid hydroxylators via CYP2D6. At the same time, the effects of metoprolol are potentiated.
Clonidine: The hypertensive reaction in the event of sudden withdrawal of clonidine can be potentiated by β-blockers. If concomitant treatment with clonidine must be discontinued, the β-blocker must be withdrawn a few days before clonidine.
Diltiazem: Diltiazem and β-receptor blockers have additive inhibitory effects on AV conduction and sinus node function. Pronounced bradycardia has been observed (case reports) in cases of combination treatment with diltiazem.
Non-steroidal anti-inflammatory drugs (NSAIDs): Anti-inflammatory drugs of the NSAID type counteract the antihypertensive effect of β-receptor blockers. Indomethacin in particular has been studied. This interaction is thought not to occur with sulindac. In a study with diclofenac no such reaction could be detected.
Phenylpropanolamine: Phenylpropanolamine (norephedrine) in single doses of 50 mg can increase diastolic blood pressure to pathological values in healthy trial subjects. Propranolol generally counteracts the rise in blood pressure induced by phenylpropanolamine. However, β-receptor blockers can cause paradoxical hypertensive reactions in patients who take high doses of phenylpropanolamine. Hypertensive crises during treatment with phenylpropanolamine alone have been described in a few cases.
Epinephrine: There have been about ten reports of marked hypertension and bradycardia in patients on treatment with non-selective β-receptor blockers (incl. pindolol and propranolol) who were given epinephrine (adrenaline). These clinical observations have been confirmed in studies on healthy trial subjects. It has also been suggested that epinephrine as an additive to local anesthetics can cause these reactions on intravascular administration. The risk is thought to be considerably less with cardio-selective β-receptor blockers.
Quinidine: Quinidine inhibits the metabolism of metoprolol in so-called rapid hydroxylators (approx. 90% in Sweden), resulting in greatly increased plasma levels and increased β-blockade. Corresponding interactions are thought to occur with other β-blockers that are metabolized by the same enzyme (cytochrome P4502D6).
Amiodarone: One case report suggests that patients treated with amiodarone may develop pronounced sinus bradycardia if they are treated concomitantly with metoprolol. Amiodarone has an extremely long half-life (approx. 50 days), which means that interactions can occur a long time after the preparation has been withdrawn.
Rifampicin: Rifampicin can induce the metabolism of metoprolol, resulting in reduced plasma levels.
Patients receiving concomitant treatment with metoprolol and other β-receptor blockers (e.g. eye drops) or MAO inhibitors should be kept under careful supervision. Inhalation anesthetics potentiate the cardiodepressive effect in patients who are being treated with β-receptor blockers. The dose of oral antidiabetic drugs may need to be adjusted for patients receiving β-blockers.
Incompatibilities: Not relevant.
Store at a temperature not exceeding 30°C.
C07FB02 - metoprolol and felodipine ; Belongs to the class of selective beta-blocking agents in combination with other antihypertensives. Used in the treatment of cardiovascular diseases.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image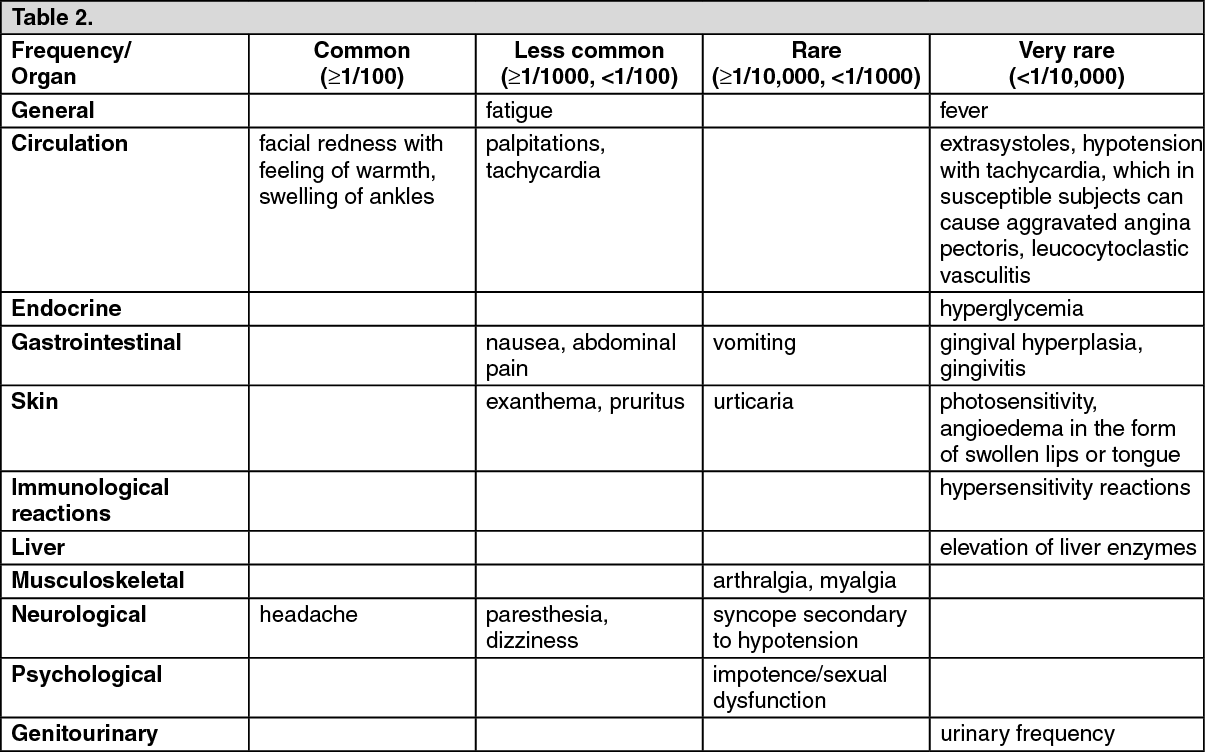 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image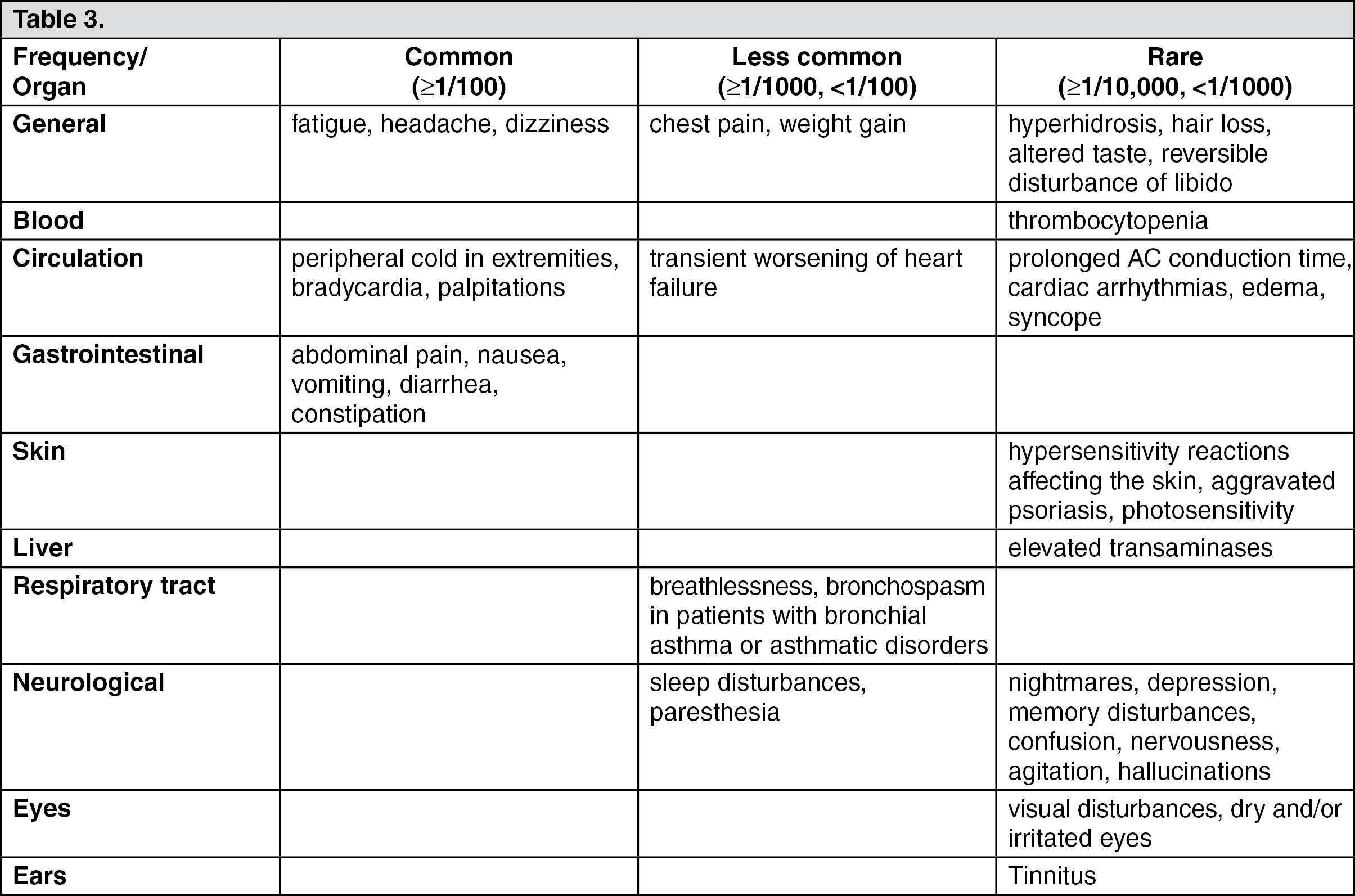 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out