Therapeutic Class: Olanzapine is an antipsychotic agent.
Pharmacology: Pharmacodynamics: Olanzapine is an antipsychotic agent that demonstrates a broad pharmacologic profile across a number of receptor systems. In preclinical studies, olanzapine exhibited affinities for serotonin 5HT
2A/2C, 5HT
3, 5HT
6; dopamine D
1, D
2, D
3, D
4, D
5; muscarinic M
1-5; adrenergic α
1; and histamine H
1 receptors. Animal behavioral studies with olanzapine indicated 5HT, dopamine and cholinergic antagonism consistent with the receptor-binding profile. Olanzapine demonstrated a greater
in vitro affinity for serotonin 5HT
2 as well as greater
in vivo serotonin 5HT
2 activity compared to dopamine D
2 receptor affinity and activity. Electrophysiological studies demonstrated that olanzapine selectively reduced the firing of mesolimbic (A10) dopaminergic neurons, while having little effect on the striatal (A9) pathways involved in motor function. Olanzapine reduced a conditioned avoidance response, a test indicative of antipsychotic activity at doses below those producing catalepsy, an effect indicative of motor side effects. Unlike some other antipsychotic agents, olanzapine increases responding in an "anxiolytic" test. In two of two placebo and two of three comparator controlled trials with over 2,900 schizophrenic patients presenting with both positive and negative symptoms, olanzapine was associated with statistically significantly greater improvements in negative as well as positive symptoms.
Mechanism of Action: Olanzapine is an atypical antipsychotic agent, is used to treat both negative and positive symptoms of schizophrenia, acute mania with bipolar disorder, agitation, and psychotic symptoms in dementia.
Pharmacokinetics: Olanzapine is well absorbed after oral administration, reaching peak plasma concentrations with 5 to 8 hours. The absorption is not affected by food. Plasma concentrations of olanzapine were linear and dose proportional in trials studying doses from 1 to 20 mg. Olanzapine is metabolized in the liver by conjugative and oxidative pathways. The major circulating metabolite is the 10-N glucuronide, which in theory does not pass the blood-brain barrier. Cytochrome P450 isoforms CYP1A2 and CYP2D6 contribute to the formation of the N-desmethyl and 2-hydrocymethyl metabolites. Both metabolites exhibited significantly less
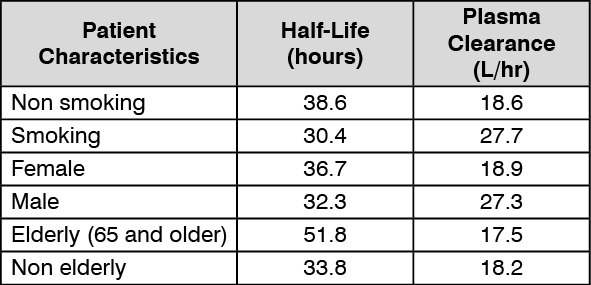
in vivo pharmacological activity than olanzapine in animal studies. The predominant pharmacologic activity is from the parent olanzapine. After oral administration to healthy subjects, the mean terminal elimination half-life was 33 hours (21 to 54 hours for 5th to 95th percentile) and the mean olanzapine plasma clearance was 26 L/hr (12 to 47 L/hr for the 5th to 95th percentile). Olanzapine pharmacokinetics varied on the basis of smoking status, gender, and age. The following summarized these effects. See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Although smoking status, gender, and to a lesser extent age may affect olanzapine clearance and half-life, the magnitude of the impact of these single factors is small in comparison to the overall variability between individuals.
Adolescents (ages 13 to 17 years): The pharmacokinetics of olanzapine are similar between adolescents and adults. In clinical studies, the average olanzapine exposure was approximately 27% higher in adolescents. Demographic differences between the adolescents and adults include a lower average body weight and fewer adolescents were smokers. Such factors likely contribute to the higher average exposure observed in adolescents. There was no significant difference in mean elimination half-life or olanzapine plasma clearance between subjects with severely impaired renal function compared to individuals with normal renal function. Approximately 57% of the radio labeled olanzapine is excreted in urine, principally as metabolites. Subjects with mild hepatic dysfunction who smoked had reduced clearance comparable to nonsmoking subjects with no hepatic dysfunction. The plasma protein binding of olanzapine was about 93% over the concentration range of about 7 to about 1000 ng/mL. Olanzapine is bound predominantly to albumin, and α1-acid glycoprotein. In a study of Caucasians, Japanese, and Chinese subjects, there were no differences in olanzapine pharmacokinetics among the three populations. Cytochrome P450 isoform CYP2D6 status does not affect the metabolism of olanzapine.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out