


 Sign Out
Sign Out


Mechanism(s) of resistance: Acquired resistance to glycopeptides is based on acquisition of various van gene complexes. Van genes have rarely been found in Staphylococcus aureus, where changes in cell wall structure result in "intermediate" susceptibility, which is most commonly heterogeneous.
There is no cross-resistance between vancomycin and other antibiotics but cross-resistance with other glycopeptide antibiotics, such as teicoplanin, does occur. Secondary development of resistance during therapy is rare.
In some countries, increasing cases of resistance are observed particularly in enterococci; multi-resistant strains of Enterococcus faecium are especially alarming.
Synergism: The combination of vancomycin with an aminoglycoside antibiotic has a synergistic effect against many strains of Staphylococcus aureus, non-enterococcal D-streptococci, enterococci and streptococci of the Viridans group. The combination of vancomycin with a cephalosporin has a synergistic effect against some oxacillin-resistant Staphylococcus epidermidis strains, and the combination of vancomycin with rifampicin has a synergistic effect against Staphylococcus epidermidis and a partial synergistic effect against some Staphylococcus aureus strains. As vancomycin in combination with a cephalosporin may also have an antagonistic effect against some Staphylococcus epidermidis strains and in combination with rifampicin against some Staphylococcus aureus strains, preceding synergism testing is useful.
Specimens for bacterial cultures should be obtained in order to isolate and identify the causative organisms and to determine their susceptibility to vancomycin.
Breakpoints: Minimum inhibitory concentration (MIC) breakpoint established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) for Staphylococcus spp. and Streptococcus spp. are Susceptible ≤2 mg/L and Resistant >2 mg/L; for Enterococcus spp. are Susceptible ≤4 mg/L and Resistant >4 mg/L; and for non-species related are Susceptible ≤2 mg/L and Resistant >4 mg/L.
Susceptibility: The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent is at least some types of infections is questionable.
Vancomycin has a narrow spectrum of action. (See table.)
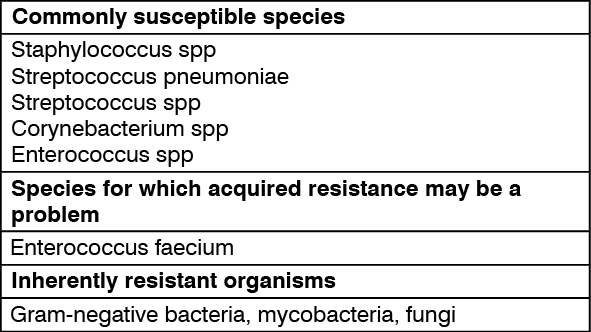 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Distribution: Following intravenous administration, vancomycin is distributed to almost all tissues and diffuses in pleural, pericardial, ascitic and synovial fluid as well as in the cardiac muscle and in heart valves. Comparable high concentrations are achieved as in blood plasma. Data about the vancomycin concentrations in bone (spongiosa, compacta) vary widely. The apparent distribution volume in steady state is stated to be 0.43 (up to 0.9) L/kg. In non-inflamed meninges vancomycin passes the blood-brain barrier only to a low extent. Vancomycin is bound to plasma proteins at 30 to 55% and even higher.
Elimination: Vancomycin is metabolized only to a low extent. After parenteral administration, it is excreted almost completely as microbiologically active substance (approx. 75-90% within 24 hours) through glomerular filtration via the kidneys. Biliary excretion is insignificant (less than 5% of a dose).
In patients with normal renal function the half-life in serum is about 4-6 (5-11) hours, in children 2.2-3 hours. In impaired renal function, the half-life of vancomycin may be considerably prolonged (up to 7.5 days). Due to ototoxicity of vancomycin therapy-adjuvant monitoring of the plasma concentrations is indicated in such cases.
Mean plasma concentrations after i.v. infusion of 1000 mg vancomycin over 60 minutes were about 63 mg/L at the end of the infusion, about 23 mg/L after 2 hours and about 8 mg/L after 11 hours.
The clearance of vancomycin from plasma correlates nearly with the glomerular filtration rate.
The total systemic and renal clearance of vancomycin can be reduced in elderly patients.
As studies in anephric patients showed, the metabolic clearance seems to be very low.
No vancomycin metabolites have been identified so far in humans.
If vancomycin is given during a peritoneal dialysis via the intraperitoneal route, approx. 60% reaches the systemic circulation during 6 hours. After i.p. administration of 30 mg/kg BW, serum levels of approx. 10 mg/l are achieved.
In case of oral use, high-polar vancomycin is virtually not absorbed. It appears after oral administration in active form in the stool, and is therefore a suitable chemotherapeutic for pseudomembranous colitis and staphylococcal colitis.
Vancomycin diffuses readily across the placenta and is distributed into cord blood.