


 Sign Out
Sign Out


 Click on icon to see table/diagram/image
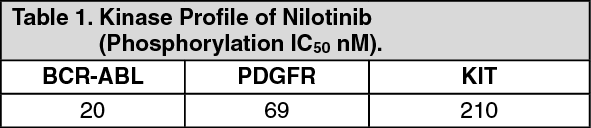
Click on icon to see table/diagram/imageMechanism of Action: Tasigna is a potent and selective inhibitor of the ABL tyrosine kinase activity of the BCR-ABL oncoprotein both in cell lines and in primary Philadelphia-chromosome positive leukemia cells. The drug binds strongly within the ATP-binding site in such a manner that it is a potent inhibitor of wild-type BCR-ABL and maintains activity against 32/33 imatinib-resistant mutant forms of BCR-ABL. As a consequence of this biochemical activity, nilotinib selectively inhibits the proliferation and induces apoptosis in BCR-ABL dependent cell lines and in primary Philadelphia-chromosome positive leukemia cells derived from CML patients. In murine models of CML, as a single agent nilotinib reduces tumor burden and prolongs survival following oral administration.
Clinical Studies: Newly Diagnosed Ph+ CML-CP: An open label, multicenter, randomized Phase III study was conducted to determine the efficacy of Tasigna versus imatinib in adult patients with cytogenetically confirmed newly diagnosed Ph+ CML-CP. Patients were within six months of diagnosis and were previously untreated for CML-CP, except for hydroxyurea and/or anagrelide. In addition, patients were stratified according to Sokal risk score at time of diagnosis.
Efficacy was based on a total of 846 patients (283 patients in the imatinib 400 mg once daily group, 282 patients in the nilotinib 300 mg twice daily group, 281 patients in the nilotinib 400 mg twice daily group).
Baseline characteristics were well balanced between the three groups. Median age was 46 years in the imatinib group and 47 years in both nilotinib groups, with 12.4%, 12.8% and 10.0% were ≥65 years of age in imatinib, nilotinib 300 mg twice daily and nilotinib 400 mg twice daily treatment groups, respectively. There were slightly more male than female patients in all groups (55.8%, 56.0% and 62.3% in imatinib, nilotinib 300 mg twice daily and nilotinib 400 mg twice daily, respectively). More than 60% of all patients were Caucasian, and 25% were Asian.
The primary data analysis time point was when all 846 patients completed 12 months of treatment (or discontinued earlier). Subsequent analyses reflect when patients completed 24, 36, 48 and 60 months of treatment (or discontinued earlier). The median time on treatment was approximately 60 months in all three treatment groups. The median actual dose intensity was 400 mg/day in the imatinib group, 593 mg/day in the nilotinib 300 mg twice daily group and 773 mg/day in the nilotinib 400 mg twice daily group. This study is on-going.
Major Molecular Response (MMR): The primary efficacy variable was MMR at 12 months after the start of study medication. MMR was defined as ≤0.1% BCR-ABL/ABL % by international scale measured by RQ-PCR, which corresponds to a ≥3 log reduction of BCR-ABL transcript from standardized baseline.
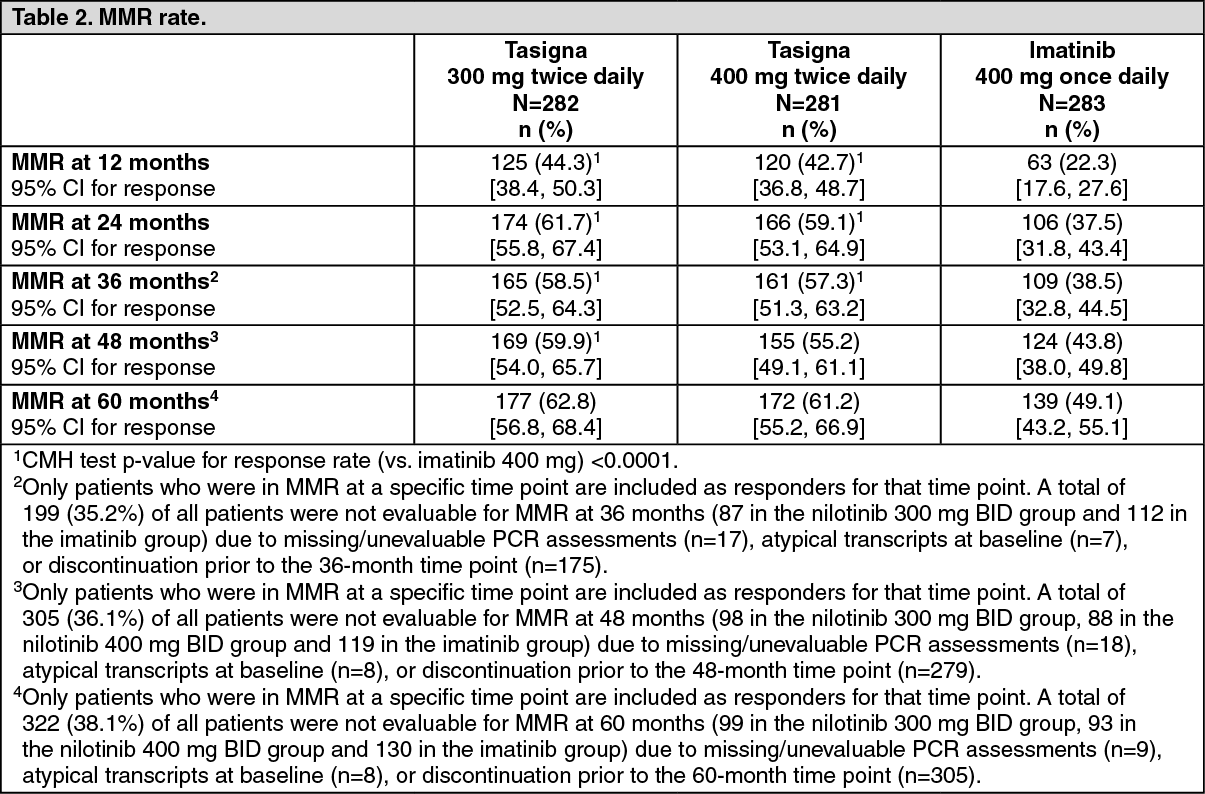
The primary efficacy endpoint, Major Molecular Response (MMR) rate at 12 months was statistically significantly superior in the nilotinib 300 mg twice daily group compared to the imatinib 400 mg once daily group (44.3% vs. 22.3%, p<0.0001). The rate of MMR at 12 months, was also statistically significantly higher in the nilotinib 400 mg twice daily group compared to the imatinib 400 mg once daily group (42.7% vs. 22.3%, p<0.0001), see Table 2.
At the nilotinib recommended dose of 300 mg twice daily, the rates of MMR at 3, 6, 9 and 12 months were 8.9%, 33.0%, 43.3% and 44.3%. In the nilotinib 400 mg twice daily group, the rates of MMR at 3, 6, 9 and 12 months were 5.0%, 29.5%, 38.1% and 42.7%. In the imatinib 400 mg once daily group, the rates of MMR at 3, 6, 9 and 12 months were 0.7%, 12.0%, 18.0% and 22.3%.
The MMR rates at 12, 24, 36, 48 and 60 months are presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
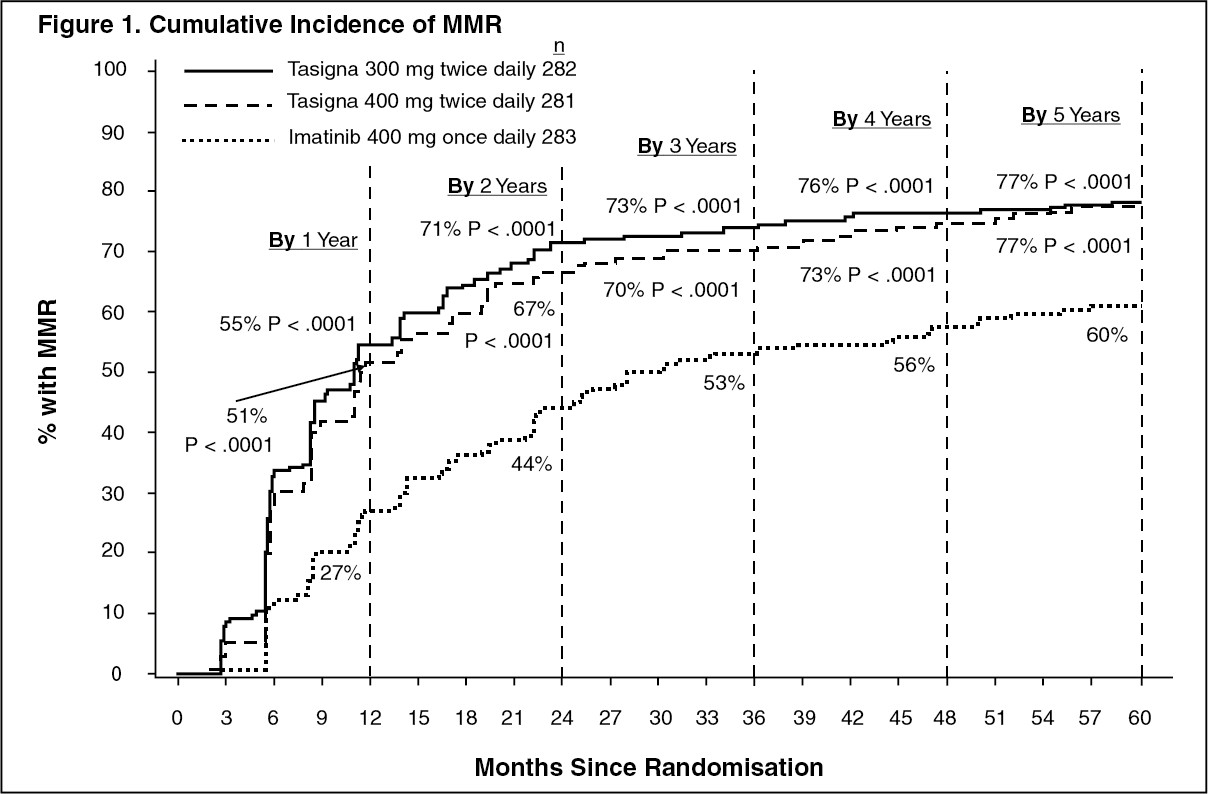
Click on icon to see table/diagram/imageMMR rates by different time points (including patients who achieved MMR at or before those time points as responders) are presented in the cumulative incidence of MMR. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor all Sokal risk groups, the MMR rates at all time points remained consistently higher in the two nilotinib groups than in the imatinib group.
In a retrospective analysis, 91% (234/258) of patients on nilotinib 300 mg twice daily achieved BCR-ABL levels ≤10% at 3 months of treatment compared to 67% (176/264) of patients on imatinib 400 mg once daily. Patients with BCR-ABL levels ≤10% at 3 months of treatment show a greater overall survival at 60 months compared to those who did not achieve this molecular response level [97% vs. 82% respectively (p=0.0116)].
Based on the Kaplan-Meier analyses of time to first MMR among all patients the probability of achieving MMR at different time points were higher in both nilotinib groups compared to the imatinib group (HR=2.20 and stratified log-rank p<0.0001 between nilotinib 300 mg twice daily and imatinib, HR=1.90 and stratified log-rank p<0.0001 between nilotinib 400 mg twice daily and imatinib).
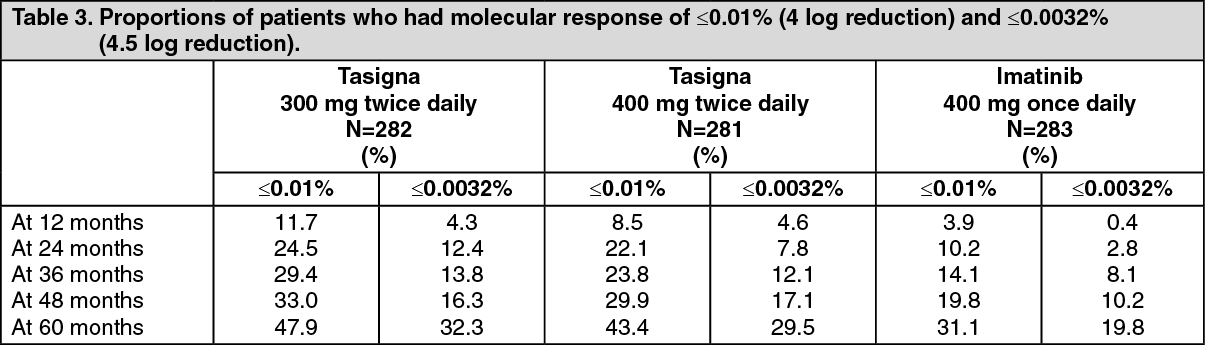
The proportions of patients who had a molecular response of ≤0.01% and ≤0.0032% by International Scale (IS) at different time-points is presented in Table 3 and the proportion of patients who had a molecular response of ≤0.01% and ≤0.0032% by IS-by different time-points are presented in Figures 2 and 3. Molecular responses of ≤0.01% and ≤0.0032% by IS corresponds to a ≥4 log reduction and ≥4.5 log reduction, respectively, of BCR-ABL transcripts from a standardized baseline. (See Table 3, Figures 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image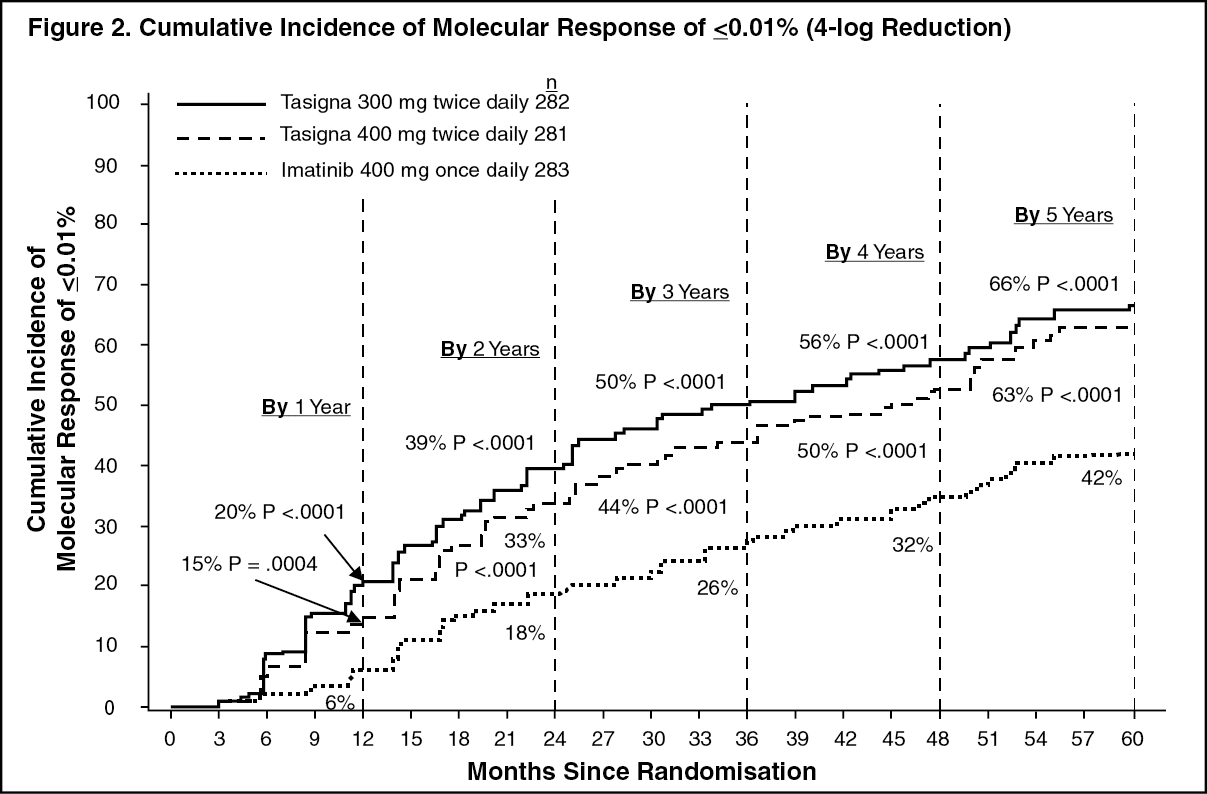 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image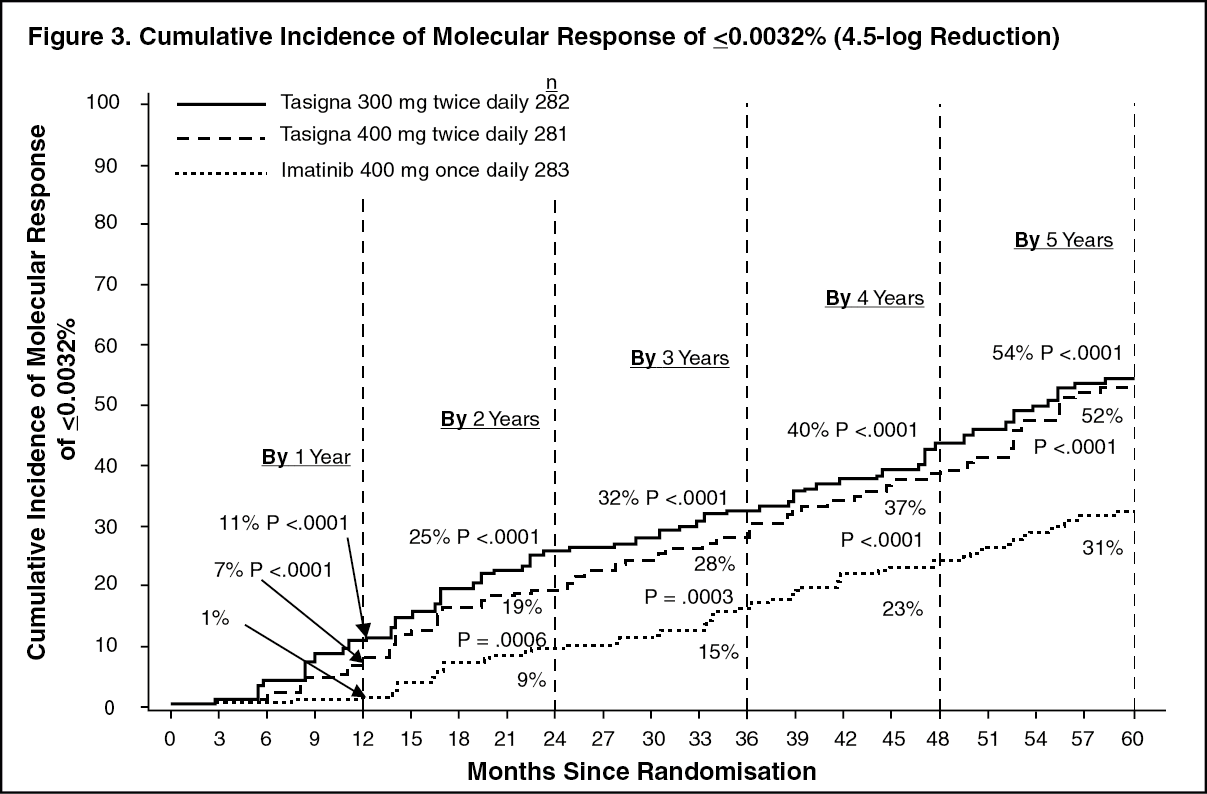 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDuration of MMR: Based on Kaplan-Meier estimates of the duration of first MMR, the proportions of patients who were maintaining response after 60 months among patients who achieved MMR were 93.4% (95% CI: 89.9% to 96.9%) in the nilotinib 300 mg twice daily group, 92.0% (95% CI: 88.2% to 95.8%) in the nilotinib 400 mg twice daily group and 89.1% (95% CI: 84.2% to 94.0%) in the imatinib 400 mg once daily group.
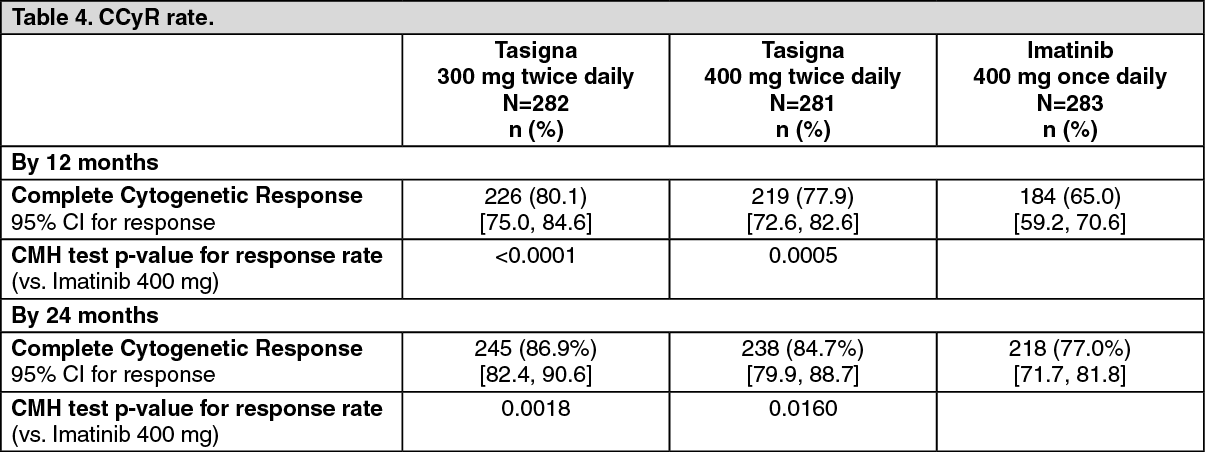
Complete Cytogenetic Response (CCyR): CCyR was defined as 0% Ph+ metaphases in the bone marrow based on a minimum of 20 metaphases evaluated. CCyR rate by 12 months (includes patients who achieved CCyR at or before the 12 month time point as responders) was statistically higher for both the nilotinib 300 mg twice daily and 400 mg twice daily groups compared to imatinib 400 mg once daily group. (See Table 4.)
CCyR rate by 24 months (includes patients who achieved CCyR at or before the 24 month time point as responders) was statistically higher for both the nilotinib 300 mg twice daily and 400 mg twice daily groups compared to imatinib 400 mg once daily group. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDuration of CCyR: Based on Kaplan-Meier estimates, the proportions of patients who were maintaining response after 60 months among patients who achieved CCyR were 99.1% (95% CI: 97.9% to 100%) in the nilotinib 300 mg twice daily group, 98.7% (95% CI: 97.1% to 100%) in the nilotinib 400 mg twice daily group and 97.0% (95% CI: 94.7% to 99.4%) in the imatinib 400 mg once daily group.
Progression to AP/BC on Treatment: Progression to AP/BC on treatment is defined as the time from the date of randomization to the first documented disease progression to AP/BC or CML-related death. Overall by the cut-off date, 17 patients progressed to AP or BC on treatment (2 in the nilotinib 300 mg twice daily group, 3 in the nilotinib 400 mg twice daily group and 12 in the imatinib 400 mg once daily group). The estimated rates of patients free from progression to AP or BC at 60 months were 99.3%, 98.7% and 95.2%, respectively (HR=0.1599 and stratified log-rank p=0.0059 between nilotinib 300 mg BID and imatinib, HR=0.2457 and stratified log-rank p=0.0185 between nilotinib 400 mg BID and imatinib). No new events of progression to AP/BC were reported on-treatment since the 2-year analysis.
Including clonal evolution as a criterion for progression, a total of 25 patients progressed to AP or BC on treatment by the cut-off date (3 in the nilotinib 300 mg twice daily group, 5 in the nilotinib 400 mg twice daily group and 17 in the imatinib 400 mg once daily group). The estimated rates of patients free from progression to AP or BC including clonal evolution at 60 months were 98.7%, 97.9% and 93.2%, respectively (HR=0.1626 and stratified log-rank p=0.0009 between nilotinib 300 mg BID and imatinib, HR=0.2848 and stratified log-rank p=0.0085 between nilotinib 400 mg BID and imatinib).
Overall Survival (OS): A total of 50 patients died during treatment or during the follow-up after discontinuation of treatment (18 in the nilotinib 300 mg twice daily group, 10 in the nilotinib 400 mg twice daily group and 22 in the imatinib 400 mg once daily group). Twenty-six (26) of these 50 deaths were related to CML (6 in the nilotinib 300 mg twice daily group, 4 in the nilotinib 400 mg twice daily group and 16 in the imatinib 400 mg once daily group). The estimated rates of patients alive at 60 months were 93.7%, 96.2% and 91.7%, respectively (HR=0.8026 and stratified log-rank p=0.4881 between nilotinib 300 mg twice daily and imatinib, HR=0.4395 and stratified log-rank p=0.0266 between nilotinib 400 mg twice daily and imatinib). Considering only CML-related deaths as events, the estimated rates of OS at 60 months were 97.7%, 98.5% and 93.8%, respectively (HR=0.3673 and stratified log-rank p=0.0292 between nilotinib 300 mg twice daily and imatinib, HR=0.2411 and stratified log-rank p=0.0057 between nilotinib 400 mg twice daily and imatinib).
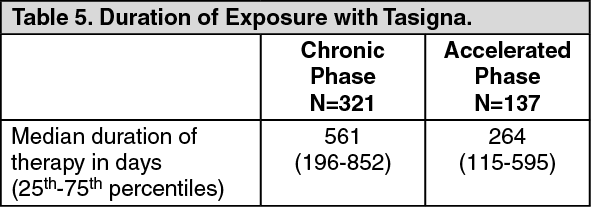
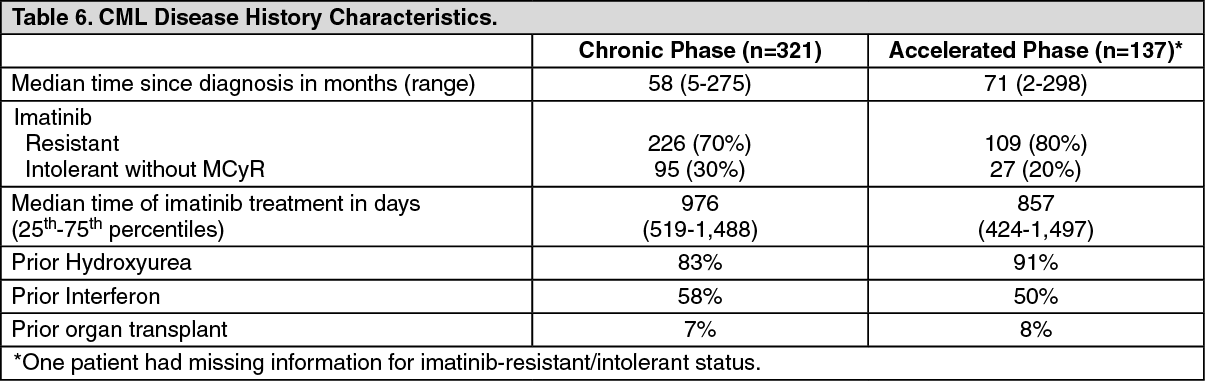
Resistant or Intolerant Ph+ CML: An open-label multicenter Phase II study was conducted to determine the efficacy of Tasigna (400 mg twice daily) in patients with imatinib resistant or intolerant CML with separate treatment arms for chronic and accelerated phase disease. Efficacy was based on 321 CP patients and 137 AP patients enrolled. Median duration of treatment was 561 days and 264 days, respectively (see Table 5). Tasigna was administered on a continuous basis, (twice daily 2 hours after a meal and no additional food for at least one hour) unless there was evidence of inadequate response or disease progression. Dose escalation to 600 mg twice daily was allowed. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageResistance to imatinib included failure to achieve a complete hematologic response (by 3 months), cytogenetic response (by 6 months) or major cytogenetic response (by 12 months) or progression of disease after a previous cytogenetic or hematologic response. Imatinib intolerance included patients who discontinued imatinib because of toxicity and were not in major cytogenetic response at time of study entry.
Overall, 73% of patients were imatinib-resistant while 27% were imatinib-intolerant. The majority of patients had a long history of CML that included extensive prior treatment with other antineoplastic agents such as imatinib, hydroxyurea, interferon, and some that had even failed stem cell transplant (Table 6). The median highest prior imatinib dose had been 600 mg/day for CP and AP patients, and the highest prior imatinib dose was ≥600 mg/day in 74% of all patients with 40% of patients receiving imatinib doses ≥800 mg/day. (See Table 6.)
 Click on icon to see table/diagram/image
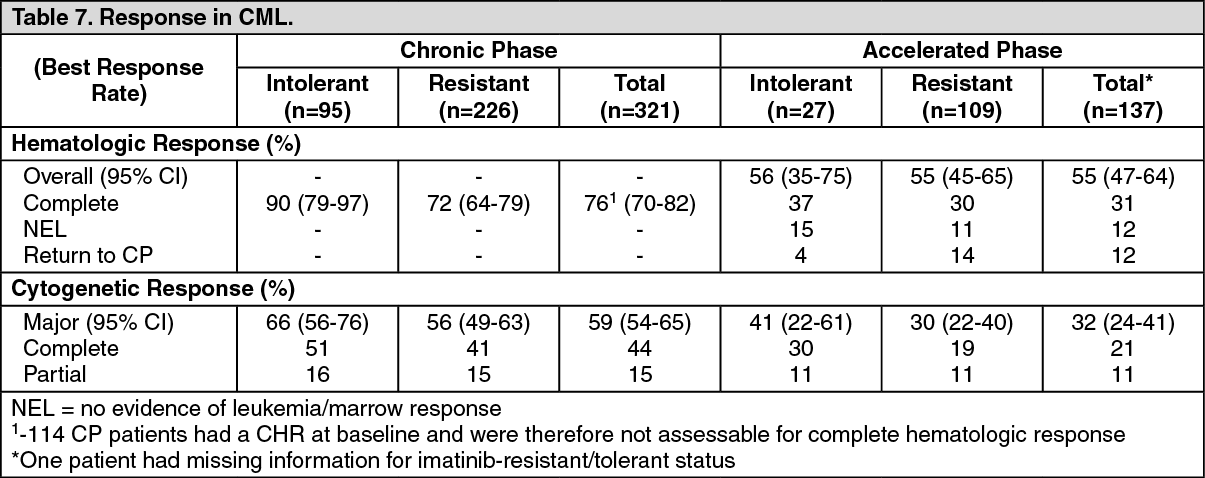
Click on icon to see table/diagram/imageThe primary endpoint in the CP patients was major cytogenetic response (MCyR), defined as elimination (CCyR, complete cytogenetic response) or significant reduction to <35% Ph+ metaphases (partial cytogenetic response) of Ph+ hematopoietic cells. Complete hematologic response (CHR) in CP patients was evaluated as a secondary endpoint. The primary endpoint in the AP patients was overall confirmed hematologic response (HR), defined as either a complete hematologic response, no evidence of leukemia or return to chronic phase.
Chronic Phase: The MCyR rate in 321 CP patients was 59%. Most responders achieved their MCyR rapidly within 3 months (median 2.8 months) of starting Tasigna treatment and these were sustained. The CCyR rate was 44%. The median time to achieve CCyR was just past 3 months (median 3.3 months). Of the patients who achieved MCyR, 77% (95% CI: 71% to 84%) were maintaining response at 24 months. Median duration of MCyR has not been reached. Of the patients who achieved CCyR, 84% (95% CI: 77% to 91%) were maintaining response at 24 months. Median duration of CCyR has not been reached. Patients with a CHR at baseline achieved a MCyR faster (1.4 vs. 2.8 months). Of CP patients without a baseline CHR, 76% achieved a CHR, median time to CHR was 1 month and median duration of CHR has not been reached.
The estimated 24-month overall survival rate in CML-CP patients was 87%.
Accelerated Phase: The overall confirmed HR rate in 137 AP patients was 55%. Most responders achieved a HR early with Tasigna treatment (median 1.0 months) and these have been durable (median duration of confirmed HR was 21.5 months). Of the patients who achieved HR, 49% (95% CI: 35% to 62%) were maintaining response at 24 months. MCyR rate was 32% with a median time to response of 2.8 months. Of the patients who achieved MCyR, 66% (95% CI: 50% to 82%) were maintaining response at 24 months. Median duration of MCyR has not been reached. The rates of response for the two treatment arms are reported in Table 7.
The estimated 24-month overall survival rate in CML-AP patients was 70%. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSeparate treatment arms were also included in the Phase II study to study Tasigna in a group of CP and AP patients who had been extensively pre-treated with multiple therapies including a tyrosine kinase inhibitor agent in addition to imatinib. Of these patients 30/36 (83%) were treatment-resistant. In 22 CP patients evaluated for efficacy Tasigna induced a 32% MCyR rate and a 50% CHR rate. In 11 AP patients evaluated for efficacy, treatment induced a 36% overall HR rate.
After imatinib failure, 24 different BCR-ABL mutations were noted in 42% of chronic phase and 54% of accelerated phase CML patients who were evaluated for mutations. Tasigna demonstrated efficacy in patients harboring a variety of BCR-ABL mutations associated with imatinib resistance, except T315I.
Pharmacokinetics: Absorption: Peak concentrations of nilotinib are reached 3 hours after oral administration. Nilotinib absorption following oral administration was approximately 30%. The absolute bioavailability of nilotinib has not been determined. As compared to an oral drink solution (pH of 1.2 to 1.3), relative bioavailablity of nilotinib capsule is approximately 50%. In healthy volunteers, Cmax and area under the concentration-time curve (AUC) of nilotinib are increased by 112% and 82%, respectively compared to fasting conditions when Tasigna is given with food. Administration of Tasigna 30 minutes or 2 hours after food increased bioavailability of nilotinib by 29% or 15%, respectively (see Dosage & Administration, Precautions and Interactions). Nilotinib absorption (relative bioavailability) might be reduced by approximately 48% and 22% in patients with total gastrectomy and partial gastrectomy, respectively.
Distribution: Blood-to-plasma ratio of nilotininb is 0.68. Plasma protein binding is approximately 98% on the basis of in vitro experiments.
Biotransformation/Metabolism: Main metabolic pathways identified in healthy subjects are oxidation and hydroxylation. Nilotinib is the main circulating component in the serum. None of the metabolites contribute significantly to the pharmacological activity of nilotinib.
Elimination: After a single dose of radiolabelled nilotinib in healthy subjects, greater than 90% of the dose was eliminated within 7 days mainly in feces. The parent drug accounted for 69% of the dose.
The apparent elimination half-life estimated from the multiple dose PK with daily dosing was approximately 17 hours. Inter-patient variability in nilotinib PK was moderate to high (% CV: 33% to 43%).
Linearity/Non-Linearity: Steady-state nilotinib exposure was dose-dependent with less than dose-proportional increases in systemic exposure at dose levels higher than 400 mg given as once daily dosing. Daily systemic exposure to nilotinib 400 mg twice-daily dosing at steady state was 35% higher than with 800 mg once-daily dosing. Systemic exposure (AUC) of nilotinib at steady state at a dose level of 400 mg twice daily was approximately 13.4% higher than with 300 mg twice daily. The average nilotinib trough and peak concentrations over 12 months were approximately 15.7% and 14.8% higher following 400 mg twice daily dosing compared to 300 mg twice daily. There was no relevant increase in exposure to nilotinib when the dose was increased from 400 mg twice-daily to 600 mg twice-daily.
Steady state conditions were essentially achieved by day 8. An increase in systemic exposure to nilotinib between the first dose and steady state was approximately 2-fold for the 400 mg once daily dosing and 3.8-fold for the 400 mg twice-daily dosing.
Bioavailability/Bioequivalence Studies: Single-dose administration of 400 mg of nilotinib, using 2 capsules of 200 mg whereby the content of each capsule was dispersed in one teaspoon of applesauce, was shown to be bioequivalent with a single dose administration of 2 intact capsules of 200 mg.
Toxicology: Non-Clinical Safety Data: Nilotinib has been evaluated in safety pharmacology, repeated dose toxicity, genotoxicity, reproductive toxicity, phototoxicity and carcinogenicity (rat and mice) studies.
Nilotinib did not have effects on CNS or respiratory functions. In vitro cardiac safety studies demonstrated a preclinical signal for QT prolongation. No effects were seen in ECG measurements in dogs or monkeys treated up to 39 weeks or in a special telemetry study in dogs.
Repeated dose toxicity studies in dogs up to 4 weeks duration and in cynomolgus monkeys up to 9 months duration, revealed the liver as the primary target organ of toxicity of nilotinib. Alterations included increased alanine aminotransferase and alkaline phosphatase activity, and histopathology findings (mainly sinusoidal cell or Kupffer cell hyperplasia/hypertrophy, bile duct hyperplasia and periportal fibrosis). In general the changes in clinical chemistry were fully reversible after a four week recovery period, the histological alterations only showed partial reversibility. Exposures at the lowest dose levels where the liver effects were seen were lower than the exposure in humans at a dose of 800 mg/day. Only minor liver alterations were seen in mice or rats treated up to 26 weeks. Mainly reversible increases in cholesterol levels were seen in rats, dogs and monkeys.
Genotoxicity studies in bacterial in vitro systems and in mammalian in vitro and in vivo systems with and without metabolic activation did not reveal any evidence for a mutagenic potential of nilotinib.
In the 2-year rat carcinogenicity study there was no evidence of carcinogenicity upon administration of nilotinib at 5, 15 and 40 mg/kg/day. Exposures (in terms of AUC) at the highest dose level were representing approximately 2x to 3x human daily steady state exposure (based on AUC) to nilotinib at the dose of 800mg/day. The major target organ for non-neoplastic lesions was the uterus (dilatation, vascular ectasia, hyperplasia endothelial cell, inflammation and/or epithelial hyperplasia).
In the 26-week Tg.rasH2 mouse carcinogenicity study, in which nilotinib was administered at 30, 100 and 300 mg/kg/day, skin papillomas/carcinomas were detected at 300 mg/kg, representing approximately 30 to 40 times (based on AUC) the human exposure at the maximum approved dose of 800 mg/day (administered as 400 mg twice daily). The No-Observed-Effect-Level for the skin neoplastic lesions was 100 mg/kg/day, representing approximately 10 to 20 times the human exposure at the maximum approved dose of 800 mg/day (administered as 400 mg twice daily). The major target organs for non-neoplastic lesions were the skin (epidermal hyperplasia), the growing teeth (degeneration/atrophy of the enamel organ of upper incisors and inflammation of the gingiva/odontogenic epithelium of incisors) and the thymus (increased incidence and/or severity of decreased lymphocytes).
Nilotinib did not induce teratogenicity, but did show embryo- and fetotoxicity at doses which also showed maternal toxicity. Increased post implantation loss was observed in both the fertility study, with treatment of both males and females, and in the embryotoxicity study with the treatment of females. Embryo-lethality and fetal effects (mainly decreased fetal weights, visceral and skeletal variations) in rats and increased resorption of fetuses and skeletal variations in rabbits were present in the embryo toxicity studies. Exposure to nilotinib in females at No-Observed-Adverse-Effect-Levels was generally less or equal to that in humans at 800 mg/day.
In a pre- and postnatal study, the oral administration of nilotinib to female rats from day 6 of gestation to day 21 or 22 postpartum resulted in maternal effects (reduced food consumption and lower body weight gains) and longer gestation period at 60 mg/kg. The maternal dose of 60 mg/kg was associated with decreased pup body weight and changes in some physical development parameters (the mean day for pinna unfolding, tooth eruption and eye opening was earlier). The No-Observed-Adverse-Effect-Level in maternal animals and offspring was a maternal dose of 20 mg/kg.
In a juvenile development study, nilotinib was administered via oral gavage to juvenile rats from the first week postpartum through young adult (day 70 postpartum) at doses of 2, 6 and 20 mg/kg/day. Effects were limited to the dose of 20 mg/kg/day and consisted of reductions in body weight parameters and food consumption with recovery after dosing ceased. The No-Observed-Effect-level in juvenile rats was considered to be 6 mg/kg/day. Overall, the toxicity profile in juvenile rats was comparable to that observed in adult rats.
Nilotinib was shown to absorb light in the UV-B and UV-A range, and to be distributed into the skin showing a phototoxic potential in vitro. However, no phototoxicity has been observed in vivo. Therefore the risk that nilotinib causes photosensitization in patients is considered very low.