Pharmacology: Pharmacodynamics: Tablet: Cefuroxime, a semi-synthetic second generation cephalosporin which exerts its bactericidal activity by interfering with the bacterial cell wall synthesis. It binds to specific penicillin-binding proteins responsible for the synthesis of peptidoglycan, a heteropolymeric structure that gives the cell wall its mechanical stability. The final stage of the peptidoglycan synthesis involves the completion of the cross-linking of the terminal glycine residue of the pentaglycine bridge to the fourth residue of the pentapeptide. The transpeptidase that catalyzes this step is inhibited by cephalosporins. As a result, the bacterial cell wall is weakened, the cell swells and then ruptures.
Powder for Injection: Cefuroxime, a semi-synthetic second generation cephalosporin, has antibacterial activity similar to penicillins, carbacephems and cephamycins. Cefuroxime exerts its bactericidal activity by interfering with the synthesis of the bacterial cell wall. It binds to specific penicillin-binding proteins responsible for the synthesis of peptidoglycan, a heteropolymeric structure that gives the cell wall its mechanical stability. The final stage of the peptidoglycan synthesis involves the completion of the cross-linking of the terminal glycine residue of the pentaglycine bridge to the fourth residue of the pentapeptide. The transpeptidase that catalyzes this step is inhibited by cephalosporins. Thus, inhibition of the transpeptidase interrupts peptidoglycan synthesis, causing formation of defective cell walls and osmotically unstable spheroplasts and lysis of the bacteria.
Pharmacokinetics: Tablet: The bioavailability of cefuroxime axetil after oral administration is variable and depends on the formulation used. The tablet/capsule formulations should not, therefore, be substituted with powder for oral suspension formulations on a mg/mg basis.
The bioavailability of cefuroxime axetil is significantly increased from 37% to 52% by coadministration with food.
Average peak serum cefuroxime concentrations of 4.1, 7, or 13.6 mcg/mL are attained approximately 2 to 3 hours after oral administration in adults of a single 250 mg, 500 mg or 1 g dose, respectively. Average serum concentrations after 6 hours are 0.7, 2.2, or 3.4 mcg/mL, respectively. The area under the curve (AUC) of the drug averaged 12.9, 27.4, or 50 mcg-hr/mL, respectively.
Cefuroxime's apparent volume of distribution in healthy adults ranges from 9.3 to 15.8 L per 1.73 m
2. Cefuroxime is widely distributed in the body including pleural fluid, sputum, bone, synovial fluid, and aqueous humor, but only achieves therapeutic concentrations in the cerebrospinal fluid when the meninges are inflamed. Cefuroxime is 33-50% protein-bound.
Cefuroxime readily crosses the placenta and can also be detected in human milk.
In adults, the serum or plasma half-life (t
1/2) after oral administration of cefuroxime axetil ranges from 1.2 to 1.6 hours and about 50% of an administered dose is recovered in the urine within 12 hours.
Following oral administration or cefuroxime axetil, the drug undergoes rapid hydrolysis by nonspecific esterases in the intestinal mucosa and blood to yield the active parent drug cefuroxime, which is released into the systemic circulation.
The axetil moiety of the drug is metabolized to acetaldehyde and acetic acid. Cefuroxime itself is not metabolized and its serum level is much closer to the minimum inhibitory concentration (MIC) of important pathogens than cefuroxime axetil.
Cefuroxime is excreted unchanged primarily in the urine by both glomerular filtration and tubular secretion.
In patients with renal impairment, the serum t
1/2 of the drug is prolonged and generally ranges from 1.9-16.1 hours depending on the degree of renal impairment.
Cefuroxime is removed by hemodialysis and by peritoneal dialysis.
500 mg: Bioequivalence Study: Cefuroxime axetil 500 mg film-coated tablet (Supplier: PT. Darya Varia Laboratoria Tbk, Indonesia).
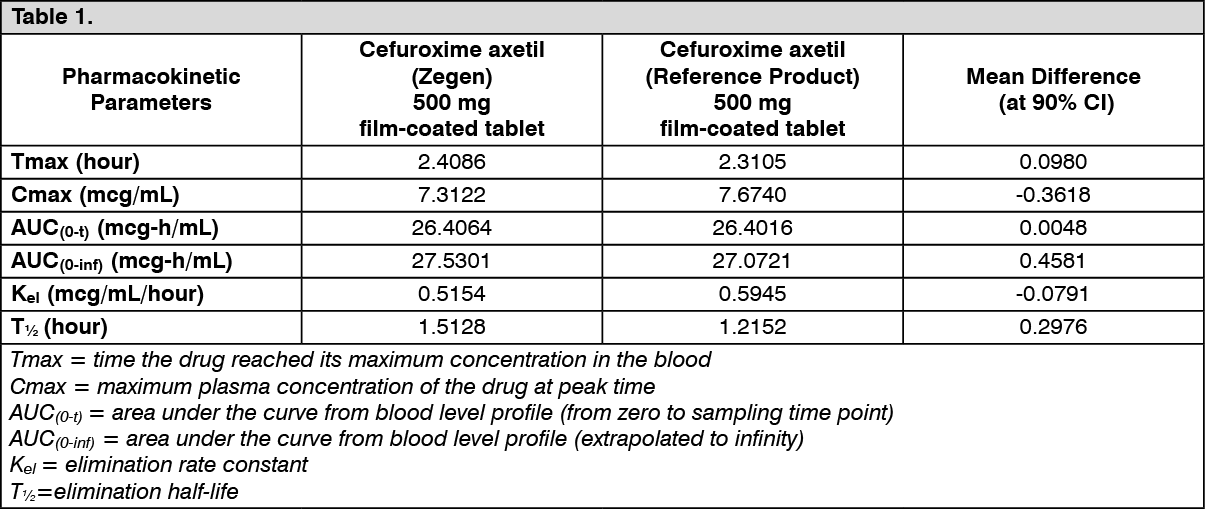
In a randomized, crossover, two-period, two-sequence design bioequivalence in-house study involving 24 healthy adult male volunteers, the bioequivalence of cefuroxime axetil (Zegen) 500 mg was compared to the reference product (innovator) of cefuroxime axetil 500 mg film-coated tablet. Volunteers were randomly allocated one tablet (fasted) to each treatment sequence and crossed over to the alternate treatment after a one-week washout period.
The following are important pharmacokinetic parameters of cefuroxime axetil in adult volunteers who received cefuroxime axetil (Zegen) and the reference product (innovator) of cefuroxime axetil 500 mg film-coated tablets (as a single oral dose): (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The study concluded that cefuroxime axetil (Zegen) 500 mg film-coated tablet by PT. Darya Varia Laboratoria Tbk, Indonesia is bioequivalent with the reference product (innovator) of cefuroxime axetil 500 mg film-coated tablet.
Powder for Injection: In neonates, a single IM administration of cefuroxime 25 mg/kg resulted in cefuroxime serum concentrations averaging 45 μg/mL, 35 μg/mL and 10.5 μg/mL 30 minutes, 3 hours, and 12 hours after injection, respectively.
Cefuroxime's serum half-life is inversely proportional to age in neonates and children. After IM or IV administration, cefuroxime's serum half-life has been reported to be 5.1 to 5.8 hours in neonates 3 days or younger, 2 to 4.2 hours in neonates 6 to 14 days, and 1 to 1.5 hours in neonates 3 to 4 weeks old.
In healthy adults with normal renal function, a single intramuscular (IM) injection of cefuroxime sodium 500-mg, 750-mg, or 1-g dose results in peak serum concentrations of 20.8 to 25.7, 26 to 34.9, and 32 to 40 μg/mL, respectively, attained within 15 to 60 minutes. A single 500- or 750-mg dose given as intravenous (IV) infusion for 30 minutes results in peak serum cefuroxime concentrations averaging 37.8 and 51.1 μg/mL, respectively.
Mean peak serum cefuroxime concentrations and areas under the concentration-time curve (AUC) attained after IM injection is almost similar to those attained after oral administration. Cefuroxime's AUC is proportional to the administered dose and is also similar after IM or IV administration.
Cefuroxime is widely distributed into body tissues and fluids including the kidneys, heart, gallbladder, liver, prostatic adenoma tissue, uterine and ovarian tissue, aqueous humor, saliva, sputum, bronchial secretions, bone, bile, adipose tissue, wound exudates, peritoneal fluid, ascitic fluid, synovial fluid, pericardial fluid, and pleural fluid after IM or IV administration. Therapeutic concentrations of cefuroxime may be attained in cerebrospinal fluid after IV administration in patients with inflamed meninges; however, only low concentrations are attained if the meninges are uninflamed.
Cefuroxime has a protein binding of 33% to 50%.
Cefuroxime readily crosses the placenta. It is also found in amniotic fluid at concentrations averaging 17 to 18.6 μg/mL after a single 750-mg IM dose. Cefuroxime is distributed in breast milk.
Microbiology: Antimicrobial Spectrum of Activity: The
in vivo bactericidal activity or cefuroxime axetil is due to the parent compound cefuroxime.
Cefuroxime has demonstrated activity against most strains of the following microorganisms both
in vitro and in clinical infections: See Table 2.
Click on icon to see table/diagram/image
Cefuroxime has also demonstrated
in vitro activity against most strains of the following microorganisms; however, clinical significance is unknown: See Table 3.
Click on icon to see table/diagram/image
Listeria monocytogenes and certain strains of enterococci, e.g.,
Enterococcus faecalis (formerly
Streptococcus faecalis), are resistant to cefuroxime. Methicillin-resistant staphylococci are resistant to cefuroxime.
Pseudomonas spp.,
Campylobacter spp.,
Acinetobacter calcoaceticus,
Legionella spp., and most strains of
Serratia spp. and
Proteus vulgaris are resistant to most first- and second-generation cephalosporins. Some strains of
Morganella morganii,
Enterobacter cloacae, and
Citrobacter spp. have been shown by
in vitro tests to be resistant to cefuroxime and other cephalosporins.
Most strains of
Clostridium difficile and
Bacteroides fragilis are resistant to cefuroxime.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image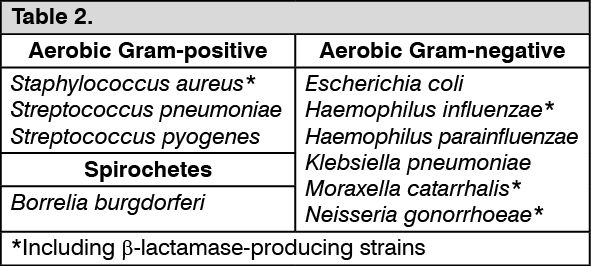 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image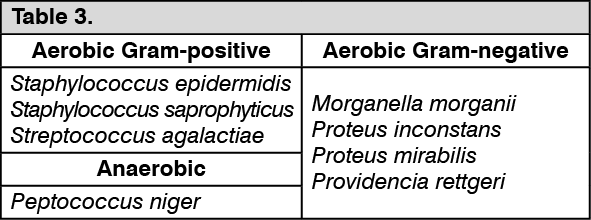 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out