


 Sign Out
Sign Out


Maintenance Therapy: While there is no body of evidence available to answer the question of how long a patient treated with aripiprazole should remain on it, systematic evaluation of patients with schizophrenia who had been symptomatically stable on other antipsychotic medication, for periods of 3 months or longer, were discontinued from those medications, and were then administered ABILIFY 15 mg/day and observed for relapse during a period of up to 26 weeks, demonstrated a benefit of such maintenance treatment [see Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Schizophrenia under Actions]. Patients should be periodically reassessed to determine the need for maintenance treatment.
Adolescents: Usual Dose: The recommended target dose of ABILIFY is 10 mg/day. Aripiprazole was studied in adolescent patients 13 to 17 years of age with Schizophrenia at daily doses of 10 mg and 30mg. The starting daily dose of the tablet formulation in these patients was 2 mg, which was titrated to 5 mg after 2 days and to the target dose of 10 mg after 2 additional days. Subsequent dose increases should be administered in 5 mg increments. The 30 mg/day dose was not shown to be more efficacious than the 10 mg/day dose and was associated with a higher incidence of significant adverse reactions including extrapyramidal disorder, somnolence and tremor [see Clinical Trials Experience under ADVERSE REACTIONS]. ABILIFY can be administered without regard to meals [see Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Schizophrenia under Actions].
Maintenance Therapy: The efficacy of ABILIFY for the maintenance treatment of schizophrenia in the adolescent population has not been evaluated. While there is no body of evidence available to answer the question of how long the adolescent patient treated with ABILIFY should be maintained on the drug, maintenance efficacy can be extrapolated from adult data along with comparisons of aripiprazole pharmacokinetic parameters in adult and paediatric patients. Thus, it is generally recommended that responding patients be continued beyond the acute response, but at the lowest dose needed to maintain remission. Patients should be periodically reassessed to determine the need for maintenance treatment.
Switching from Other Antipsychotics: There are no systematically collected data to specifically address switching patients with schizophrenia from other antipsychotics to ABILIFY or concerning concomitant administration with other antipsychotics. While immediate discontinuation of the previous antipsychotic treatment may be acceptable for some patients with schizophrenia, more gradual discontinuation may be most appropriate for others. In all cases, the period of overlapping antipsychotic administration should be minimized.
Bipolar Disorder: Acute Treatment of Manic and Mixed Episodes: Adults: The recommended starting dose in adults is 15 mg given once daily as monotherapy and 10 to 15 mg given once daily as adjunctive therapy with lithium or valproate. ABILIFY can be given without regard to meals. The recommended target dose of ABILIFY is 15 mg/day, as monotherapy or as adjunctive therapy with lithium or valproate. The dose may be increased to 30 mg/day based on clinical response. The safety of doses above 30 mg/day has not been evaluated in clinical trials.
Adolescents: The recommended starting dose in adolescent patients as monotherapy is 2 mg/day, with titration to 5 mg/day after 2 days, and a target dose of 10 mg/day after 2 additional days. Subsequent dose increases, if needed, should be administered in 5 mg/day increments. ABILIFY can be given without regard to meals. Enhanced efficacy at doses higher than a daily dose of 10 mg has not been demonstrated, and a daily dose of 30 mg is associated with a substantially higher incidence of significant adverse reactions including extrapyramidal disorder, somnolence, akathisia and salivary hypersecretion. Doses higher than 10 mg/day should therefore only be used in exceptional cases and with close clinical monitoring [see Extrapyramidal symptoms (EPS) under PRECAUTIONS, Clinical Trials Experience under ADVERSE REACTIONS, and Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Bipolar Disorder under Actions]. Younger patients are at increased risk of experiencing adverse events associated with aripiprazole. Therefore, ABILIFY is not recommended for use in patients below 13 years of age [see Clinical Trials Experience under ADVERSE REACTIONS and Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Bipolar Disorder under Actions].
Maintenance Therapy: The recommended dose for maintenance treatment is the same dose needed to stabilize patients during acute treatment, both for adult and paediatric patients. Systematic evaluation of adult patients with Bipolar I Disorder experiencing a manic or mixed episode, who had been symptomatically stable on ABILIFY Tablets (15 mg/day or 30 mg/day with a starting dose of 30 mg/day) for 6 consecutive weeks and then randomized to ABILIFY Tablets (15 mg/day or 30 mg/day) or placebo for at least 6 months and up to an additional 17 months of observation for relapse, demonstrated a benefit of such maintenance treatment [see Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Bipolar Disorder under Actions]. Patients should be periodically reassessed to determine the need for maintenance treatment.
Adjunctive Treatment of Major Depressive Disorder: The recommended starting dose for ABILIFY as adjunctive treatment for patients already taking an antidepressant is 2 to 5 mg/day. The recommended dosage range is 2 to 15 mg/day. Dosage adjustments of up to 5 mg/day should occur gradually, at intervals of no less than 1 week [see Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Adjunctive Treatment of Major Depressive Disorder under Actions]. Patients should be periodically reassessed to determine the continued need for maintenance treatment.
Irritability Associated with Autistic Disorder: Paediatric Patients (6 to 17 years): The recommended dosage range for the treatment of paediatric patients with irritability associated with autistic disorder is 5 to 15 mg/day.
Dosing should be initiated at 2 mg/day. The dose should be increased to 5 mg/day, with subsequent increases to 10 or 15 mg/day if needed. Dose adjustments of up to 5 mg/day should occur gradually, at intervals of no less than 1 week [see Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Irritability Associated with Autistic Disorder under Actions]. Patients should be periodically reassessed to determine the continued need for maintenance treatment.
Tourette's Disorder: Paediatric Patients (6 to 18 years): The recommended dosage range for Tourette's Disorder is 5 to 20 mg/day.
For patients weighing less than 50 kg, dosing should be initiated at 2 mg/day with a target dose of 5 mg/day after 2 days. The dose can be increased to 10 mg/day in patients who do not achieve optimal control of tics. Dosage adjustments should occur gradually at intervals of no less than 1 week.
For patients weighing 50 kg or more, dosing should be initiated at 2 mg/day for 2 days, and then increased to 5 mg/day for 5 days, with a target dose of 10 mg/day on day 8. The dose can be increased up to 20 mg/day for patients who do not achieve optimal control of tics. Dosage adjustments should occur gradually in increments of 5 mg/day at intervals of no less than 1 week [see Pharmacology: Pharmacodynamics: CLINICAL STUDIES: Tourette's Disorder under Actions].
Patients should be periodically reassessed to determine the continued need for maintenance treatment.
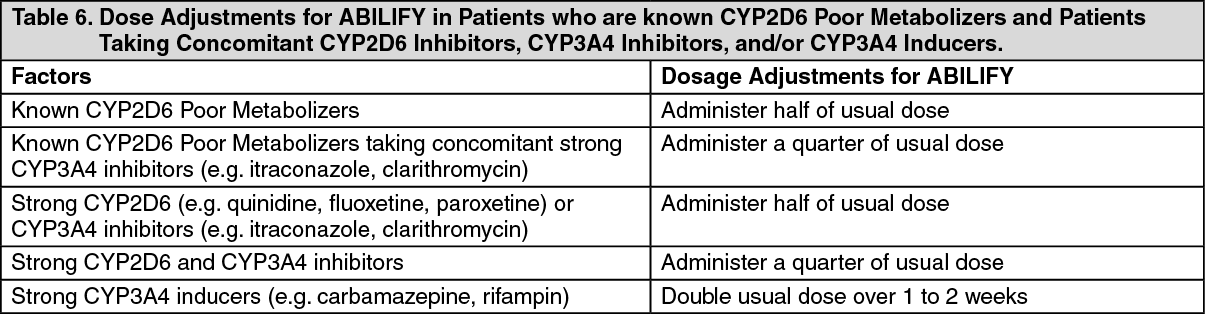
Dosage Adjustments for Cytochrome P450 Considerations: Dosage adjustments are recommended in patients who are known CYP2D6 poor metabolizers and in patients taking concomitant CYP3A4 inhibitors or CYP2D6 inhibitors or strong CYP3A4 inducers (see Table 6). When the co-administered drug is withdrawn from the combination therapy, ABILIFY dosage should then be adjusted to its original level. When the co-administered CYP3A4 inducer is withdrawn, ABILIFY dosage should be reduced to the original level over 1 to 2 weeks. Patients who may be receiving a combination of strong, moderate, and weak inhibitors of CYP3A4 and CYP2D6 (e.g., a strong CYP3A4 inhibitor and a moderate CYP2D6 inhibitor or a moderate CYP3A4 inhibitor with a moderate CYP2D6 inhibitor), the dosing may be reduced to one-quarter (25%) of the usual dose initially and then adjusted to achieve a favourable clinical response. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen adjunctive ABILIFY is administered to patients with major depressive disorder, ABILIFY should be administered without dosage adjustment as specified in Adjunctive Treatment of Major Depressive Disorder as previously mentioned.
Dosing of Oral Solution: The oral solution can be substituted for tablets on an mg-per-mg basis up to the 25 mg dose level. Patients receiving 30 mg tablets should receive 25 mg of the solution [see PHARMACOLOGY: Pharmacokinetics under Actions].