


 Sign Out
Sign Out

The most common ADRs (incidence ≥1/10 and suspected to be related to treatment by the investigator) from the pooled safety data were (in decreasing order): stomatitis, rash, fatigue, diarrhoea, infections, nausea, decreased appetite, anaemia, dysgeusia, pneumonitis, oedema peripheral, hyperglycaemia, asthenia, pruritus, weight decreased, hypercholesterolaemia, epistaxis, cough and headache.
The most common grade 3/4 ADRs (incidence ≥1/100 to <1/10 and suspected to be related to treatment by the investigator) were stomatitis, anaemia, hyperglycaemia, fatigue, infections, pneumonitis, diarrhoea, asthenia, thrombocytopenia, neutropenia, dyspnoea, lymphopenia, proteinuria, haemorrhage, hypophosphataemia, rash, hypertension, aspartate aminotransferase (AST) increased, alanine aminotransferase (ALT) increased, pneumonia and diabetes mellitus.
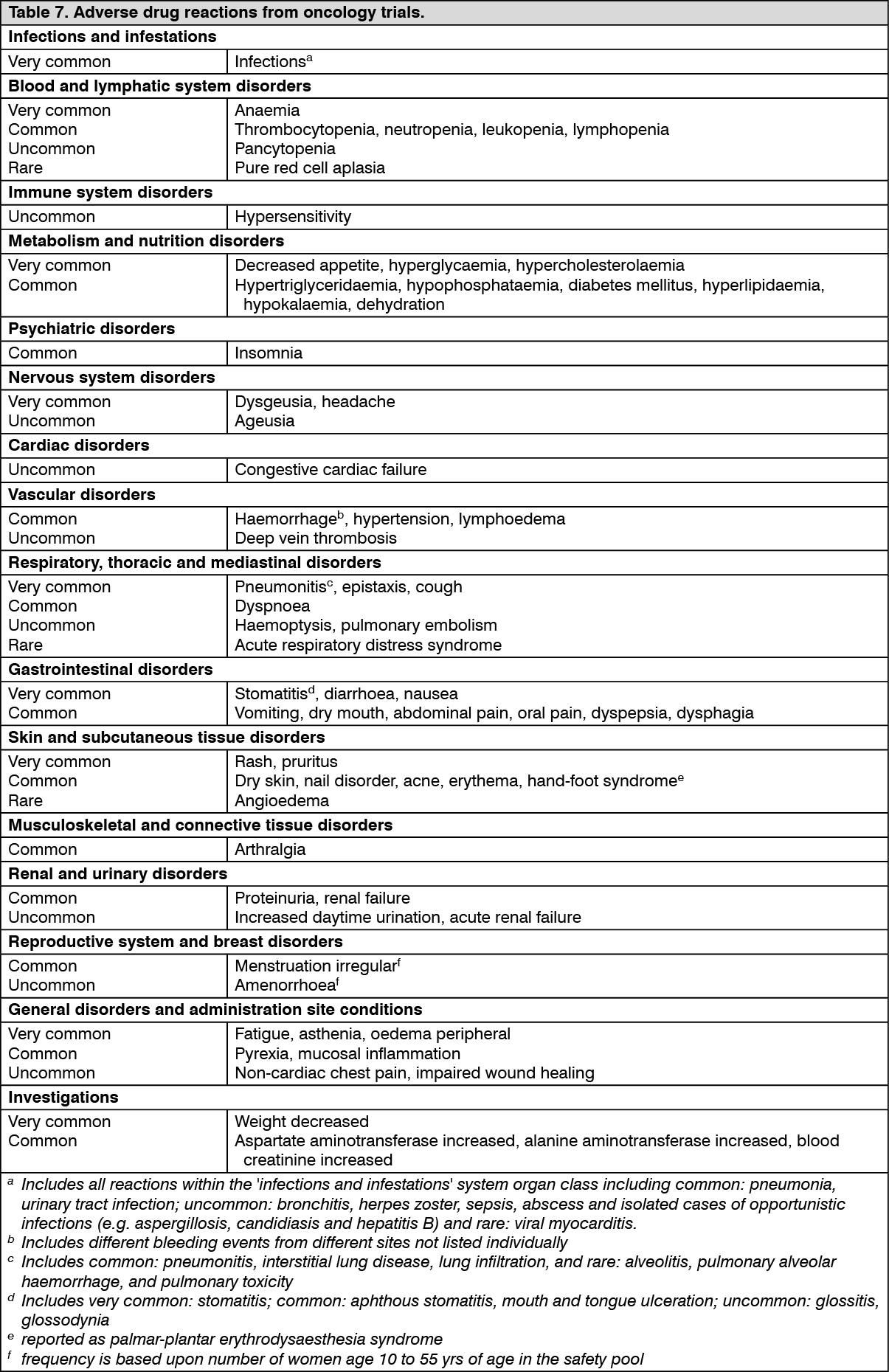
Tabulated summary of adverse drug reactions from clinical trials in oncology: Table 7 presents the frequency category of ADRs reported in the pooled safety analysis.
ADRs are listed according to MedDRA system organ class. Within each system organ class, the ADRs are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, ADRs are presented in order of decreasing frequency. In addition, the corresponding frequency category using the following convention (CIOMS III) very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinically relevant laboratory abnormalities: In the pooled double-blind phase III safety database, the following new or worsening clinically relevant laboratory abnormalities were reported with an incidence of ≥1/10 (very common, listed in decreasing frequency): Haematology: haemoglobin decreased, lymphocytes decreased, white blood cells decreased, platelet count decreased, and neutrophils decreased (or collectively as pancytopenia).
Clinical chemistry: glucose (fasting) increased, cholesterol increased, triglycerides increased, AST increased, phosphate decreased, ALT increased, creatinine increased, potassium decreased and albumin decreased.
Most of the observed abnormalities (≥1/100) were mild (grade 1) or moderate (grade 2).
Grade 3/4 haematology and chemistry abnormalities include: Haematology: lymphocytes decreased, haemoglobin decreased, (very common); neutrophils decreased, platelet count decreased, white blood cells decreased (all common).
Clinical chemistry: glucose (fasting) increased (very common); phosphate decreased, potassium decreased, AST increased, ALT increased, creatinine increased, cholesterol (total) increased, triglycerides increased, albumin decreased (all common).
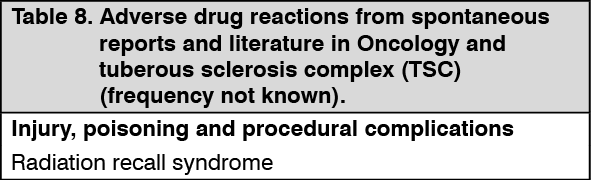
Adverse drug reactions from spontaneous reports and literature cases (frequency not known): The following adverse drug reactions have been derived from post-marketing experience with Afinitor via spontaneous case reports and literature cases. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency which is therefore categorized as not known. Adverse drug reactions are listed according to system organ classes in MedDRA. Within each system organ class, ADRs are presented in order of decreasing seriousness. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse drug reactions: In clinical trials and post-marketing spontaneous reports, everolimus has been associated with serious cases of hepatitis B reactivation, including fatal outcome. Reactivation of infections is an expected event during periods of immunosuppression (see Precautions).
In clinical trials and post-marketing spontaneous reports, everolimus has been associated with renal failure events (including fatal outcome) and proteinuria. Monitoring of renal function is recommended (see Precautions).
In clinical trials and post-marketing spontaneous reports, everolimus has been associated with cases of amenorrhea (including secondary amenorrhea).
In clinical trials and post-marketing spontaneous reports, everolimus has been associated with pneumocystis jirovecii pneumonia (PJP), some with fatal outcome (see Precautions).
In clinical trials and post-marketing spontaneous reports, angioedema has been reported with and without concomitant use of ACE inhibitors (see Precautions).
In a post-marketing single arm study in postmenopausal women with advanced hormone receptor-positive, HER2-negative breast cancer (N=92), topical treatment with dexamethasone 0.5 mg/5 mL alcohol-free oral solution (10 mL swished in the mouth for 2 minutes and then spat out, to be repeated 4 times daily for 8 weeks) was administered as a mouthwash to patients at the time of initiating treatment with Afinitor (10 mg/day) plus exemestane (25 mg/day) to reduce the incidence and severity of stomatitis. No food or drink was to be consumed for at least 1 hour after swishing and spitting the dexamethasone oral solution. The incidence of grade ≥2 stomatitis at 8 weeks was 2.4% (n=2/85 evaluable patients) which was lower than historically reported at 27.4% (n=132/482) in the phase III study in this patient population (BOLERO-2). The incidence of grade 1 stomatitis was 18.8% (n=16/85) and no grade 3 or 4 stomatitis were reported. The overall safety profile in this study was consistent with that established for everolimus in the oncology and TSC settings, with the exception of oral candidiasis which was reported in 2.2% (n=2/92) of patients in this study compared to 0.2% (n=1/482) of patients in BOLERO-2.
Special populations: Geriatric patients (65 years of age or older): In the pooled oncology safety database, 37% of the Afinitor-treated patients were ≥65 years of age.
The number of oncology patients with an ADR leading to discontinuation of Afinitor was higher in patients ≥65 years of age (20% vs. 13%). The most common ADRs (≥1/100) leading to discontinuation were pneumonitis (including interstitial lung disease), stomatitis, fatigue and dyspnea.
View ADR Monitoring Form