


 Sign Out
Sign Out

Pharmacology: Mechanism of action: Everolimus is an inhibitor targeting mTOR (mammalian target of rapamycin), or more specifically, mTORC1 (mammalian 'target of rapamycin' complex 1). It exerts its activity through high affinity interaction with the intracellular receptor protein FKBP12. The FKBP12/everolimus complex binds to mTORC1, inhibiting its signaling capacity. mTOR is a key serine-threonine kinase playing a central role in the regulation of cell growth, proliferation and survival. The regulation of mTORC1 signaling is complex, being modulated by mitogens, growth factors, energy and nutrient availability. mTORC1 is an essential regulator of global protein synthesis downstream on the PI3K/AKT pathway, which is dysregulated in the majority of human cancers.
mTORC1 signaling is effected through modulation of the phosphorylation of downstream effectors, the best characterized of which are the translational regulators S6 ribosomal protein kinase (S6K1) and eukaryotic initiation factor 4E-binding protein (4E-BP1). Disruption of S6K1 and 4E-BP1 function, as a consequence of mTORC1 inhibition, interferes with the translation of mRNAs encoding pivotal proteins involved in cell cycle regulation, glycolysis and adaptation to low oxygen conditions (hypoxia). This inhibits tumor growth and expression of hypoxia-inducible factors (e.g. HIF-1 transcription factors); the latter resulting in reduced expression of factors involved in the potentiation of tumor angiogenic processes (e.g. the vascular endothelial growth factor VEGF) in multiple tumors such as RCC and angiomyolipoma). Two primary regulators of mTORC1 signaling are the oncogene suppressors tuberin-sclerosis complexes 1 & 2 (TSC1, TSC2). Loss or inactivation of either TSC1 or TSC2 leads to elevated rheb-GTP levels, a ras family GTPase, which interacts with the mTORC1 complex to cause its activation. mTORC1 activation leads to a downstream kinase signaling cascade, including activation of the S6K1. A substrate of mTOR complex 1 (mTORC1), S6K1 phosphorylates the estrogen receptor, which is responsible for ligand-independent receptor activation.
Everolimus is a potent inhibitor of the growth and proliferation of tumor cells, endothelial cells, fibroblasts and blood vessel-associated smooth muscle cells. Consistent with the central regulatory role of mTORC1, everolimus has been shown to reduce tumor cell proliferation, glycolysis and angiogenesis in solid tumors in vivo, and thus provides two independent mechanisms for inhibiting tumor growth: direct antitumor cell activity and inhibition of the tumor stromal compartment.
Activation of the mTOR pathway is a key adaptive change driving endocrine resistance in breast cancer. Various signal transduction pathways are activated to escape the effect of endocrine therapy. One pathway is the PI3K/Akt/mTOR pathway, which is constitutively activated in aromatase inhibitor (AI)-resistant and long-term estrogen-deprived breast cancer cells. In vitro studies show that estrogen-dependent and HER2+ breast cancer cells are sensitive to the inhibitory effects of everolimus, and that combination treatment with everolimus and aromatase inhibitors enhances the anti-tumor activity of everolimus in a synergistic manner. In breast cancer cells, resistance to AIs due to Akt activation can be reversed by co-administration with everolimus.
Pharmacodynamics: There was a moderate correlation between the decrease in the phosphorylation of 4E-BP1 (P4E-BP1) in tumor tissue and the average everolimus Cmin at steady state in blood after daily administration of 5 or 10 mg everolimus. Further data suggest that the inhibition of phosphorylation of the S6 kinase is very sensitive to the mTOR inhibition by everolimus. Inhibition of phosphorylation of elF-4G was complete at all Cmin values after the 10 mg daily dose.
A trend suggestive of longer progression-free survival with higher time-normalized everolimus Cmin (defined as (area under the Cmin-time curve from study start to the time of the event)/(time from study start to the event)) was evident in patients with advanced pancreatic neuroendocrine tumors (pNET, risk ratio 0.73; 95% CI: 0.50 to 1.08) and in patients with advanced carcinoid tumor (risk ratio 0.66; 95% CI: 0.40 to 1.08). Everolimus Cmin impacted the probability of tumor size reduction (p<0.001) with the odds ratios of 1.62 and 1.46, respectively, for a change in exposure from 5 ng/mL to 10 ng/mL in patients with advanced pNET and in patients with advanced carcinoid tumor.
Clinical Studies: Hormone receptor-positive advanced breast cancer: BOLERO-2 (Study CRAD001Y2301), a randomized, double-blind, multicenter phase III study of Afinitor + exemestane versus placebo + exemestane was conducted in postmenopausal women with estrogen receptor-positive, HER 2-neu/non-amplified advanced breast cancer with recurrence or progression following prior therapy with letrozole or anastrozole. Patients were randomized in a 2:1 ratio to receive either everolimus (10 mg daily) or matching placebo in addition to open-label exemestane (25 mg daily). Randomization was stratified by documented sensitivity to prior hormonal therapy (yes vs. no) and by the presence of visceral metastasis (yes vs. no). Sensitivity to prior hormonal therapy was defined as either (1) documented clinical benefit (complete response [CR], partial response [PR], stable disease ≥24 weeks) to at least one prior hormonal therapy in the advanced setting or (2) at least 24 months of adjuvant hormonal therapy prior to recurrence.
The primary endpoint for the trial was progression-free survival (PFS) evaluated by Response Evaluation Criteria in Solid Tumors (RECIST), based on the investigators (local radiology) assessment. Supportive PFS analyses were based on an independent central radiology review.
Secondary endpoints included overall survival (OS), Overall Response Rate (ORR), Clinical Benefit Rate (CBR), Safety, change in Quality of Life (QoL) and time to ECOG PS deterioration. Additional endpoints included changes in bone turnover markers at 6 and 12 weeks.
A total of 724 patients were randomized in 2:1 ratio to the combination everolimus (10 mg daily) + exemestane (25 mg daily) (n=485) or placebo + exemestane arm (25 mg daily) (n=239). The two treatment groups were generally balanced with respect to the baseline demographics of disease characteristics and history of prior anti-neoplastic usages. The median age of patients was 61 years (range 28 to 93) and 75% were Caucasian. The median duration of blinded treatment was 24 weeks for patients receiving Afinitor plus exemestane and 13.4 weeks for those receiving placebo plus exemestane.
The efficacy results were obtained from the final analysis of PFS after 510 local PFS events and 320 central PFS events were observed. Patients in the placebo + exemestane arm did not cross-over to everolimus at the time of progression.
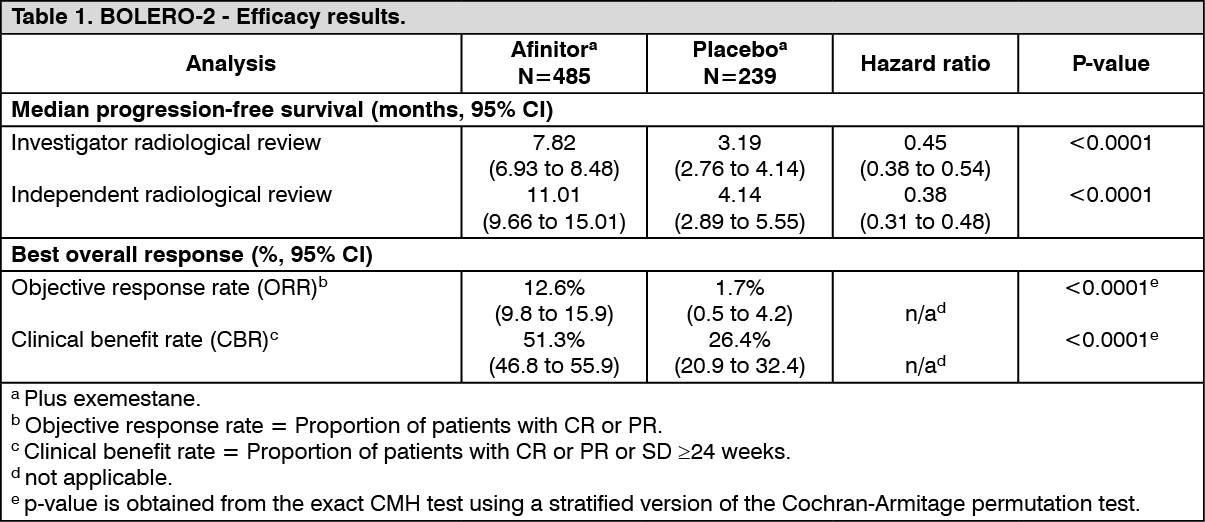
The study demonstrated a statistically significant clinical benefit of everolimus + exemestane over placebo + exemestane by a 2.5-fold prolongation in median PFS (median: 7.82 months versus 3.19 months), resulting in a 55% risk reduction of progression or death (PFS HR 0.45; 95% CI: 0.38, 0.54; one-sided log-rank test p-value <0.0001 per local investigator assessment (see Table 1).
The analysis of PFS based on independent central radiological assessment was supportive and showed a 2.7-fold prolongation in median progression-free-survival (11.01 months versus 4.14 months), resulting in a 62% risk reduction of progression or death (PFS HR 0.38; 95% CI: 0.31, 0.48; one-sided log-rank test p-value<0.0001) (see Table 1).
Objective response as per investigator assessment based on RECIST was observed in 12.6% of patients (95% CI: 9.8, 15.9) in the everolimus + exemestane arm vs. 1.7% (95% CI: 0.5-4.2) in the placebo + exemestane arm (p<0.0001 for comparison between arms). Clinical benefit rate for everolimus + exemestane was 51.3% vs. 26.4% in the control arm; p<0.0001 (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt the time of the final overall survival (OS) analysis, the median duration of OS was 31 months versus 26.6 months for the everolimus + exemestane arm versus the placebo + exemestane arm, respectively [HR=0.89 (95% CI: 0.73 to 1.10; p=0.1426)].
Twelve-month PFS rates were 33% of patients receiving everolimus + exemestane compared with 11% in the placebo + exemestane arm.
The estimated PFS treatment effect was supported by planned subgroup analysis of PFS per investigator assessment. For all analyzed subgroups, (e.g. age group (<65 years and ≥65 years), region, race, # of organs involved, # of prior therapies, sensitivity to prior hormonal therapy, presence of visceral metastasis, prior chemotherapy, bone only lesions at baseline, baseline ECOG performance status, PgR status and prior use of hormonal therapy other than NSAI) a positive treatment effect was seen with everolimus + exemestane with an estimated hazard ratio vs. placebo + exemestane ranging from 0.25 to 0.62. Subgroup analyses demonstrated a homogeneous and consistent treatment effect irrespective of sensitivity to prior hormonal therapy and presence of visceral metastasis, and across major demographic and prognostic subgroups.
Tumor reduction was also evident in 70.8% of patients in the everolimus + exemestane arm versus 29.7% for placebo + exemestane.
Clinically or statistically significant differences were not observed between the two treatment arms in terms of time to deterioration of ECOG PS (≥1 point) and median times to deterioration (≥5%) of QLQ-C30 domain scores.
Effects on bone: There are no long-term data on the effect of everolimus on bone. Comparative data from BOLERO-2 showed marked improvement in serum bone-turnover markers during the first 12 weeks of therapy, suggesting a favorable effect on bone turnover.
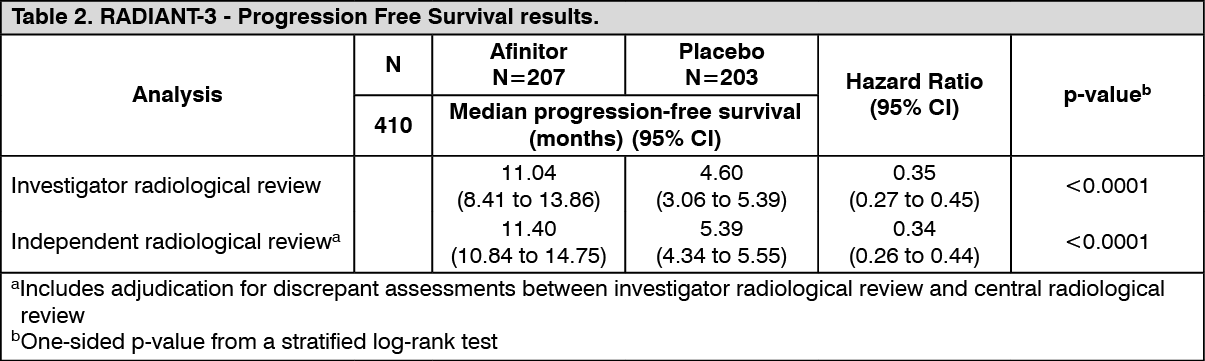
Advanced neuroendocrine tumors of gastrointestinal, lung or pancreatic origin: RADIANT-3 (Study CRAD001C2324), a randomized, double-blind, multicenter phase III study of Afinitor plus best supportive care (BSC) versus placebo plus BSC in patients with advanced pancreatic neuroendocrine tumors (pNET), demonstrated a statistically significant clinical benefit of Afinitor over placebo by a 2.4-fold prolongation in median progression-free-survival PFS (11.04 months versus 4.6 months), resulting in a 65% risk reduction in PFS (HR 0.35; 95% CI: 0.27, 0.45; p<0.0001) (see Table 2).
RADIANT-3 enrolled patients with advanced pNET whose disease had progressed within the prior 12 months. Patients were stratified by prior cytotoxic chemotherapy (yes/no) and by WHO performance status (0 vs. 1 and 2). Treatment with somatostatin analogs was allowed as part of BSC.
The primary endpoint for the trial was PFS evaluated by RECIST (Response Evaluation Criteria in Solid Tumors, version 1.0) as per investigator radiology review. After documented radiological progression, patients could be unblinded by the investigator: those randomized to placebo were then able to receive open-label Afinitor.
Secondary endpoints include safety, objective response rate ORR (complete response (CR) or partial response (PR)), response duration, and overall survival OS.
In total, 410 patients were randomized 1:1 to receive either Afinitor 10 mg/day (n=207) or placebo (n=203). Demographics were well balanced (median age 58 years, 55% male, 78.5% Caucasian). Median duration of blinded study treatment was 37.8 weeks for patients receiving Afinitor and 16.1 weeks for those receiving placebo. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEighteen-months PFS rates were 34.2% for Afinitor therapy compared to 8.9% for placebo.
The objective response rate per investigator assessment was 4.8% for the everolimus arm vs. 2.0% for the placebo arm. Tumor reduction was also evident in 64.4% of patients in the everolimus arm versus 20.6% for placebo.
At the time of the final overall survival (OS) analysis, the median duration of OS was 44 months for the everolimus arm versus 37.7 months for the placebo arm, respectively [HR=0.94 (95% CI: 0.73 to 1.20)]; p=0.300. Following disease progression, crossover to open-label Afinitor occurred in 172 of 203 patients (84.7%) randomized to placebo and may have confounded the detection of any treatment-related difference in overall survival.
RADIANT-4 (Study CRAD001T2302), a randomized, double-blind, multicenter phase III study of Afinitor plus best supportive care (BSC) versus placebo plus best supportive care was conducted in patients with advanced non-functional neuroendocrine tumors (NET) of gastrointestinal or lung origin without a history of and no active symptoms related to carcinoid syndrome. Randomization was stratified by prior somatostatin analog (SSA) use, tumor origin and WHO performance status.
The primary endpoint for the study was progression-free survival (PFS) evaluated by Response Evaluation Criteria in Solid Tumors (modified RECIST version 1.0), based on independent radiological assessment. Supportive PFS analysis was based on local investigator review.
Secondary endpoints included overall survival (OS), Overall Response Rate (ORR), Disease Control Rate (DCR=proportion of patients with a best overall response of complete response, partial response or stable disease), Safety, change in Quality of Life (QoL) via FACT-G and time to WHO PS deterioration.
A total of 302 patients were randomized in a 2:1 ratio to receive either everolimus (10 mg daily) (n=205) or placebo (n=97). The two treatment groups were generally balanced with respect to the baseline demographics, disease characteristics and history of prior somatostatin analog (SSA) use. The median age of patients was 63 years (range 22 to 86) and 76% were Caucasian. The median duration of blinded treatment was 40.4 weeks for patients receiving Afinitor and 19.6 weeks for those receiving placebo. Patients in the placebo arm did not cross-over to everolimus at the time of progression.
The efficacy results were obtained from the final analysis of PFS after 178 PFS events were observed per independent radiological review.
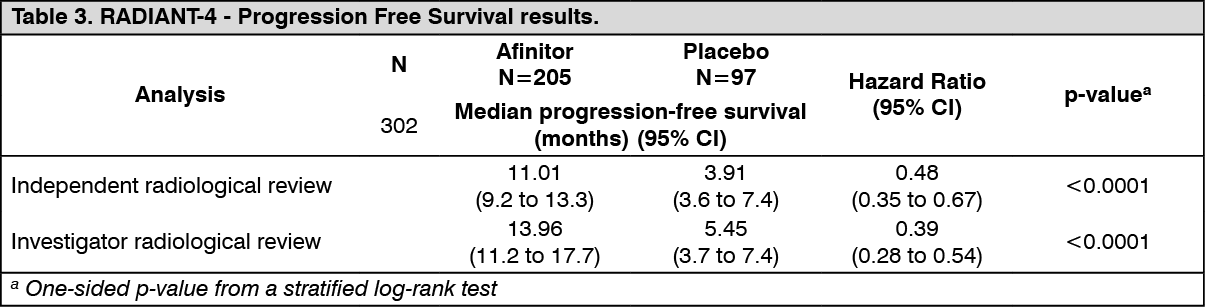
The study demonstrated a statistically significant clinical benefit of everolimus over placebo by a 2.8-fold prolongation in median PFS (11.01 months versus 3.91 months), resulting in a 52% risk reduction of progression or death (HR 0.48; 95% CI: 0.35, 0.67; one-sided stratified log-rank test p-value <0.0001) per independent assessment (see Table 3).
The analysis of PFS based on local investigator assessment was supportive and showed a 2.5-fold prolongation in median progression-free-survival (13.96 months versus 5.45 months), resulting in a 61% risk reduction of progression or death (HR 0.39; 95% CI: 0.28, 0.54; one-sided stratified log-rank test p-value<0.0001) (see Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe overall PFS benefit favored Afinitor across predefined demographic and prognostic stratification subgroups (e.g., prior SSA treatment, tumor origin grouping and WHO performance status) and with a hazard ratio range of 0.43 to 0.63). A post-hoc subgroup analysis of PFS showed a positive PFS benefit for sites of tumor origin by gastrointestinal [HR=0.60 (95% CI: 0.39 to 0.91)], lung [HR=0.50 (95% CI: 0.28 to 0.88)] and carcinoma of unknown primary/other origin [HR=0.50 (95% CI: 0.22 to 1.16)].
The overall response rate as per independent assessment was 2% in the everolimus arm vs. 1% in the placebo arm. Disease control rate (CR or PR or SD) for everolimus was 82.4% vs. 64.9% in the placebo arm. Tumor reduction was also evident indicating that 63.6% of patients in the everolimus arm experienced tumor shrinkage versus 25.9% for placebo.
The overall survival (OS) analysis is not yet mature. At the first interim analysis, 42 (20.5%) deaths were observed in the Afinitor arm vs. 28 (28.9%) deaths in the placebo arm; however the results of this analysis did not meet the pre-specified stopping boundary for statistical significance [HR= 0.64 (95% CI: 0.40 to 1.05; p=0.037)].
Clinically or statistically significant differences were not observed between the two treatment arms in terms of time to deterioration of WHO PS (≥1 point) and time to deterioration of FACT-G total score (≥7 points).
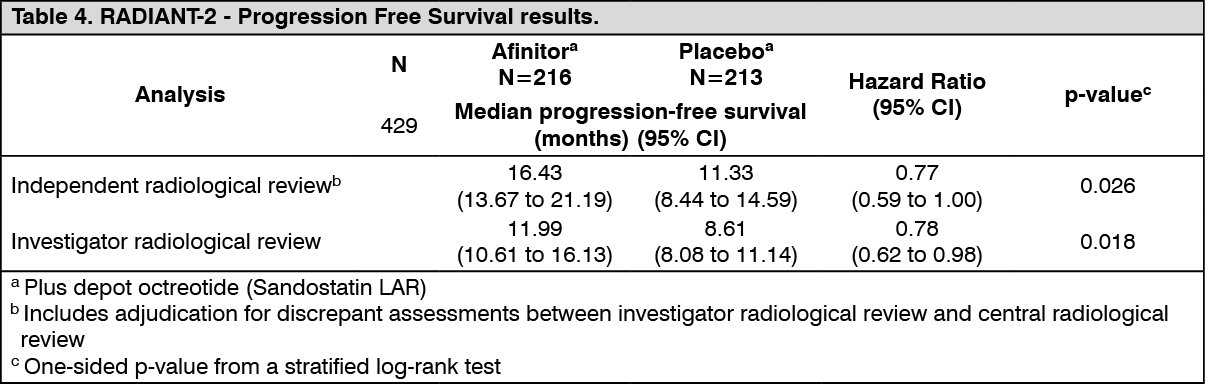
RADIANT-2 (Study CRAD001C2325), a randomized, double-blind, multicenter phase III study of Afinitor plus depot octreotide (Sandostatin LAR) versus placebo plus depot octreotide in patients with advanced neuroendocrine tumors (carcinoid tumor) primarily of gastrointestinal or lung origin showed evidence of clinical benefit of Afinitor over placebo by a 5.1-month prolongation in median PFS (16.43 months versus 11.33 months; HR 0.77; 95% CI: 0.59 to 1.00; one-sided p=0.026), resulting in a 23% risk reduction in primary PFS (see Table 4). Although statistical significance was not reached for the primary analysis (boundary for statistical significance was p=0.0246), analyses which adjusted for informative censoring and imbalances in the two treatment arms showed a treatment effect in favor of everolimus.
RADIANT-2 enrolled patients with advanced neuroendocrine tumors (carcinoid tumor) primarily of gastrointestinal or lung origin whose disease had progressed within the prior 12 months and had a history of secretory symptoms. 80.1% of the patients in the Afinitor group received somatostatin analog therapy prior to study entry compared to 77.9% in the placebo group.
The primary endpoint is PFS evaluated by RECIST as per independent radiological review. After documented radiological progression, patients could be unblinded by the investigator: those randomized to placebo were then able to receive open-label Afinitor.
Secondary endpoints include safety, objective response, response duration, and overall survival.
In total, 429 patients were randomized 1:1 to receive either Afinitor 10 mg/day (n=216) or placebo (n=213), in addition to depot octreotide (Sandostatin LAR, administered intramuscularly) 30 mg every 28 days. Median duration of blinded study treatment was 37.0 weeks for patients receiving Afinitor and 36.6 weeks for those receiving placebo. Notable imbalances were evident for several important baseline prognostic factors, mainly in favor of the placebo group. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional analyses for independent radiological review which adjusted for informative censoring and imbalances in the two treatment arms showed a treatment effect in favor of everolimus. Results of an additional adjusted multivariate analysis which corrected for imbalances between treatment arms yielded a HR of 0.73 (95% CI: 0.56 to 0.97). A Cox model with Inverse Probability of Censoring Weights (IPCW) was used to address and correct for informative censoring and imbalances in baseline characteristics between the two study arms. The estimated HR (95% CI) from the IPCW analysis was 0.60 (0.44 to 0.84) in favor of Afinitor.
Eighteen-months PFS rates were 47.2% for everolimus therapy plus depot octreotide (Sandostatin LAR) compared with 37.4% for placebo plus depot octreotide (Sandostatin LAR).
The objective response rate per independent radiological review was 2.3% for the everolimus plus depot octreotide (Sandostatin LAR) arm vs. 1.9% for the placebo plus depot octreotide (Sandostatin LAR) arm. Tumor reduction was also evident in 75.0% of patients in the everolimus plus depot octreotide (Sandostatin LAR) arm versus 44.8% in the placebo plus depot octreotide (Sandostatin LAR) arm.
The final analysis of overall survival did not show a statistically significant difference in OS (HR =1.16; (95% CI: 0.91 to 1.49)). There were 133 (61.6%) deaths in the everolimus plus depot octreotide arm and 120 (56.3%) in the placebo plus depot octreotide arm. Crossover of >58% of patients from placebo to open-label Afinitor following disease progression, imbalance between treatment arms in subsequent use of octreotide and imbalance of key prognostic factors at baseline likely confounded the detection of any treatment-related difference in OS. When adjusted for important prognostic factors, the OS hazard ratio inclined towards unity (HR 1.06; 95% CI: 0.82, 1.36).
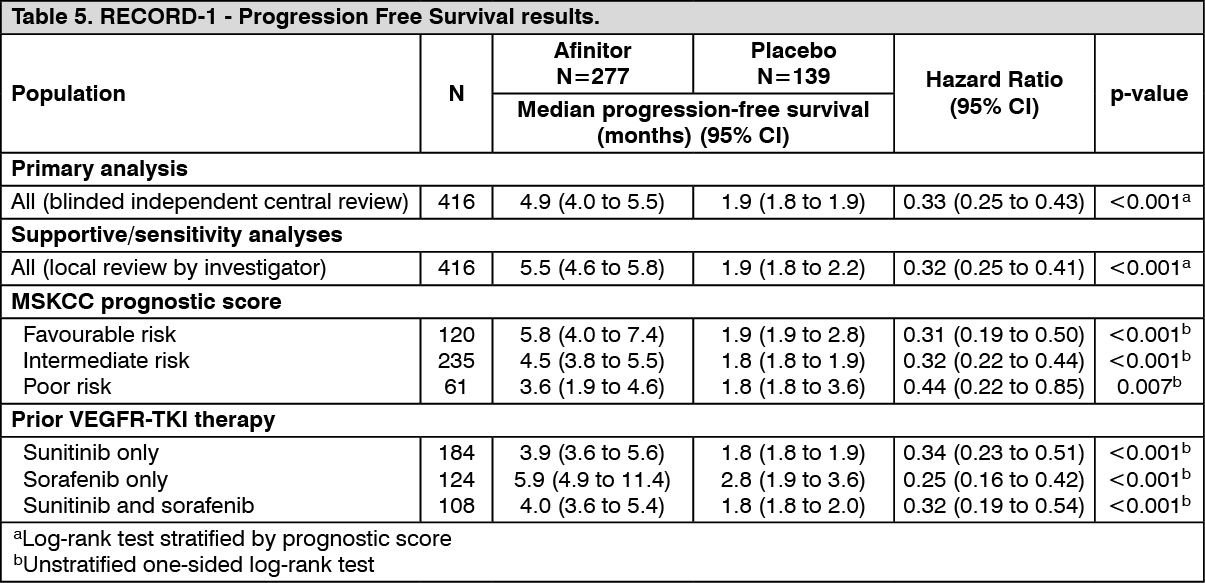
Advanced renal cell carcinoma: RECORD-1 (CRAD001C2240), a phase III, international, multicenter, randomized, double-blind study comparing Afinitor 10 mg/day and placebo, both in conjunction with best supportive care, was conducted in patients with metastatic renal cell carcinoma whose disease had progressed despite prior treatment with VEGFR-TKI (vascular endothelial growth factor receptor tyrosine kinase inhibitor) therapy (sunitinib, sorafenib, or both sunitinib and sorafenib). Prior therapy with bevacizumab and interferon-alpha was also permitted. Patients were stratified according to Memorial Sloan-Kettering Cancer Center (MSKCC) prognostic score (favourable- vs. intermediate- vs. poor-risk groups) and prior anticancer therapy (1 vs. 2 prior VEGFR-TKIs).
Progression-free survival, documented using RECIST (Response Evaluation Criteria in Solid Tumors) and assessed via a blinded, independent central review, was the primary endpoint. Secondary endpoints included safety, objective tumor response rate, overall survival, disease-related symptoms, and quality of life. After documented radiological progression, patients could be unblinded by the investigator: those randomized to placebo were then able to receive open-label Afinitor 10 mg/day. The Independent Data Monitoring Committee recommended termination of this trial at the time of the second interim analysis as the primary endpoint had been met.
In total, 416 patients were randomized 2:1 to receive Afinitor (n=277) or placebo (n=139). Demographics were well balanced (pooled median age 61 years [range 27 to 85], 77% male, 88% Caucasian, 74% one prior VEGFR-TKI therapy). Median duration of blinded study treatment was 141 days for patients receiving Afinitor and 60 days for those receiving placebo.
Results from a planned interim analysis showed that Afinitor was superior to placebo for the primary endpoint of progression-free survival, with a statistically significant 67% reduction in the risk of progression or death (see Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSix-month PFS rates were 36% for Afinitor therapy compared with 9% for placebo.
Confirmed objective tumor responses were observed in 5 patients (2%) receiving Afinitor while none were observed in patients receiving placebo. The progression-free survival advantage therefore primarily reflects the population with disease stabilization (corresponding to 67% of the Afinitor treatment group).
Final overall survival results yielded a trend in favor of Afinitor; the difference between treatment arms was not statistically significant (HR 0.90; 95% CI: 0.71 to 1.14; p=0.183). Crossover to open-label Afinitor following disease progression occurred in 111 of 139 patients (79.9%) allocated to placebo and may have confounded the detection of any treatment-related difference in overall survival. A strong trend is evident supporting better quality of life among patients receiving Afinitor as measured by disease-related symptoms (HR 0.75; 95% CI: 0.53 to 1.06; p=0.053).
Pharmacokinetics: Absorption: After administration of Afinitor Tablets in patients with advanced solid tumors, peak everolimus concentrations are reached 1 to 2 hours after administration of an oral dose of 5 to 70 mg everolimus under fasting conditions or with a light fat-free snack. Cmax is dose-proportional with daily dosing between 5 and 10 mg. With single doses of 20 mg and higher, the increase in Cmax is less than dose-proportional, however AUC shows dose-proportionality over the 5 to 70 mg dose range.
Food Effect: In healthy subjects, high fat meals reduced systemic exposure to 10 mg Afinitor Tablets (as measured by AUC) by 22% and the peak blood concentration Cmax by 54%. Low-fat meals reduced AUC by 32% and Cmax by 42%.
Distribution: The blood-to-plasma ratio of everolimus, which is concentration-dependent over the range of 5 to 5,000 ng/mL, is 17% to 73%. The amount of everolimus confined to the plasma is approximately 20% at blood concentrations observed in cancer patients given Afinitor 10 mg/day. Plasma protein binding is approximately 74% both in healthy subjects and in patients with moderate hepatic impairment.
Following intravenous administration in a rat model, everolimus was shown to cross the blood-brain barrier in a non-linear dose-dependent manner, suggesting saturation of an efflux pump at the blood-brain barrier. Brain penetration of everolimus has also been demonstrated in rats receiving oral doses of everolimus.
Biotransformation/metabolism: Everolimus is a substrate of CYP3A4 and PgP. Following oral administration, it is the main circulating component in human blood. Six main metabolites of everolimus have been detected in human blood, including three monohydroxylated metabolites, two hydrolytic ring-opened products, and a phosphatidylcholine conjugate of everolimus. These metabolites were also identified in animal species used in toxicity studies, and showed approximately 100-times less activity than everolimus itself. Hence, the parent substance is considered to contribute the majority of the overall pharmacological activity of everolimus.
Elimination: No specific excretion studies have been undertaken in cancer patients; however, data are available from the transplantation setting. Following the administration of a single dose of radiolabelled everolimus in conjunction with ciclosporin, 80% of the radioactivity was recovered from the faeces, while 5% was excreted in the urine. The parent substance was not detected in urine or faeces
Steady-state pharmacokinetics: After administration of Afinitor Tablets in patients with advanced solid tumors, steady-state AUC0-τ was dose-proportional over the range of 5 to 10 mg with a daily dosing regimen. Steady-state was achieved within two weeks. Cmax is dose-proportional between 5 and 10 mg daily. Tmax occurs at 1 to 2 hours post-dose. There was a significant correlation between AUC0-τ and pre-dose trough concentration at steady-state on a daily regimen. The mean elimination half-life of everolimus is approximately 30 hours.
Special populations: Hepatic impairment: The safety, tolerability and pharmacokinetics of Afinitor were evaluated in two single oral dose studies of Afinitor Tablets in subjects with impaired hepatic function relative to subjects with normal hepatic function. In one study the average AUC of everolimus in 8 subjects with moderate hepatic impairment (Child-Pugh class B) was twice that found in 8 subjects with normal hepatic function. In a second study of 34 subjects with different impaired hepatic function compared to normal subjects, there was a 1.6-fold, 3.3-fold, and 3.6-fold increase in exposure (i.e. AUC(0-inf)) for subjects with mild (Child-Pugh A), moderate (Child-Pugh B), and severe (Child-Pugh C) hepatic impairment, respectively. Simulations of multiple dose pharmacokinetics support the dosing recommendations in hepatic impaired subjects based on their Child Pugh status.
Based on a meta-analysis of the two studies, dose adjustment is recommended for patients with hepatic impairment (see Precautions and Dosage & Administration).
Renal impairment: In a population pharmacokinetic analysis of 170 patients with advanced cancer, no significant influence of creatinine clearance (25 to 178 mL/min) was detected on CL/F of everolimus. Post-transplant renal impairment (creatinine clearance range 11 to 107 mL/min) did not affect the pharmacokinetics of everolimus in transplant patients.
Pediatric patients (below 18 years): There is no indication for use of Afinitor in the pediatric cancer population (see Dosage & Administration).
Geriatric patients (65 years of age or older): In a population pharmacokinetic evaluation in cancer patients, no significant influence of age (27 to 85 years) on oral clearance (CL/F: range 4.8 to 54.5 litres/hour) of everolimus was detected.
Race/Ethnicity: Oral clearance (CL/F) is similar in Japanese and Caucasian cancer patients with similar liver functions.
Based on analysis of population pharmacokinetics, oral clearance (CL/F) is on average 20% higher in black transplant patients.
Toxicology: Non-clinical Safety Data: The preclinical safety profile of everolimus was assessed in mice, rats, minipigs, monkeys and rabbits. The major target organs were male and female reproductive systems (testicular tubular degeneration, reduced sperm content in epididymides and uterine atrophy) in several species; lungs (increased alveolar macrophages) in rats and mice; and eyes (lenticular anterior suture line opacities) in rats only. Minor kidney changes were seen in the rat (exacerbation of age-related lipofuscin in tubular epithelium, increases in hydronephrosis) and mouse (exacerbation of background lesions). There was no indication of kidney toxicity in monkeys or minipigs.
Everolimus appeared to spontaneously exacerbate background diseases (chronic myocarditis in rats, coxsackie virus infection of plasma and heart in monkeys, coccidian infestation of the gastrointestinal tract in minipigs, skin lesions in mice and monkeys). These findings were generally observed at systemic exposure levels within the range of therapeutic exposure or above, with the exception of the findings in rats, which occurred below therapeutic exposure due to a high tissue distribution.
In juvenile rat toxicity studies at doses as low as 0.15 mg/kg/day, systemic toxicity included decreased body weight gain and food consumption, and delayed attainment of some developmental landmarks at all doses, with full or partial recovery after cessation of dosing. With the possible exception of the rat-specific lens finding, where young animals appeared to be more susceptible, it appears that there is no significant difference in the sensitivity of juvenile animals to the adverse effects of everolimus as compared to adult animals at doses of 0.5 to 5 mg/kg per day. No relevant toxicity was evident in juvenile monkeys at doses up to 0.5 mg/kg/day for 4-weeks.
Genotoxicity studies covering relevant genotoxicity endpoints showed no evidence of clastogenic or mutagenic activity. Administration of everolimus for up to 2 years did not indicate any oncogenic potential in mice and rats up to the highest doses, corresponding respectively to 3.9 and 0.2 times the estimated clinical exposure from a 10 mg daily dose.
Reproductive toxicity: For information on reproductive toxicity, see Use in Pregnancy & Lactation.