


 Sign Out
Sign Out
Patient selection for treatment of RET-gene fusion (NSCLC or thyroid cancer) or a RET-gene mutation (MTC) should be based on a validated test method.
Posology: The recommended dose is 400 mg pralsetinib once daily on an empty stomach (see Method of administration as follows). Treatment should be continued until disease progression or unacceptable toxicity.
If vomiting occurs after taking a dose of pralsetinib, the patient should not take an additional dose but continue with the next scheduled dose.
Missed doses: If a dose of pralsetinib is missed, the patient should make up for the missed dose as soon as possible on the same day. The regular daily dose schedule for pralsetinib should be resumed the next day.
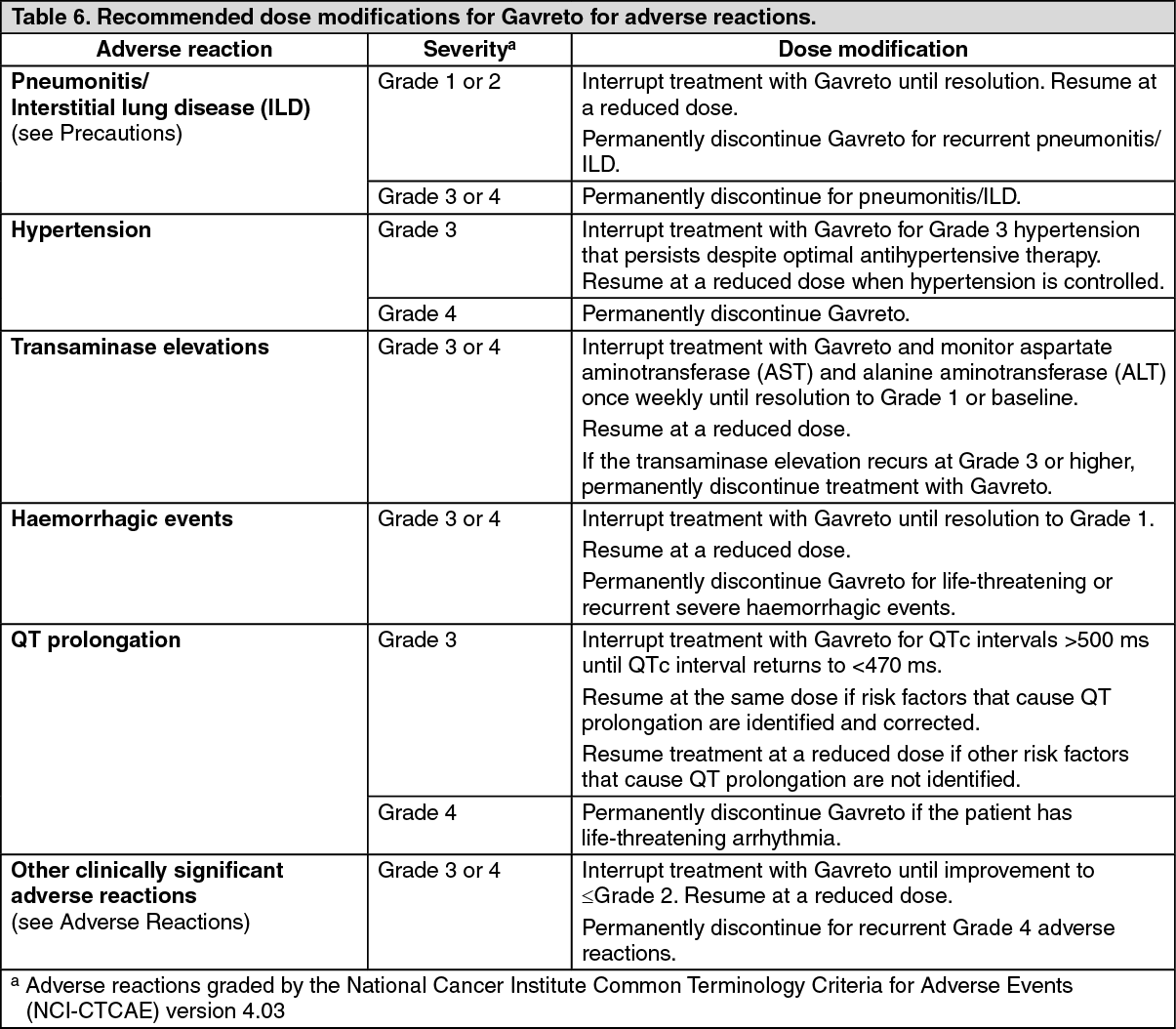
Dose modifications for adverse reactions: Interruption of treatment with or without dose reduction may be considered to manage adverse reactions based on severity and clinical presentation.
Patients may have their dose reduced by 100 mg decrements to a minimum dose of 100 mg once daily. Gavreto should be permanently discontinued in patients who are unable to tolerate 100 mg orally once daily.
Recommended dose modifications for adverse reactions are indicated in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
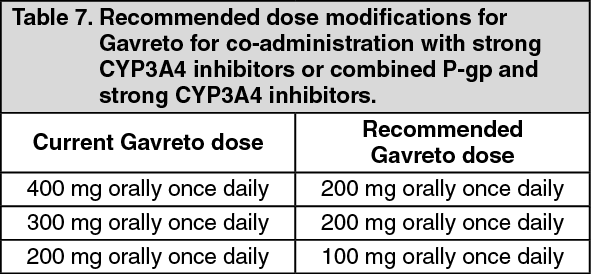
Click on icon to see table/diagram/imageDose modification for use with strong cytochrome P-450 (CYP)3A4 inhibitors or combined P-glycoprotein (P-gp) and strong CYP3A4 inhibitors: Concomitant use of pralsetinib with known strong CYP3A4 inhibitors or combined P-gp and strong CYP3A4 inhibitors should be avoided (see Precautions and Interactions). If co-administration with a strong CYP3A4 inhibitor or combined P-gp and strong CYP3A4 inhibitor cannot be avoided, the current dose of pralsetinib should be reduced as recommended in Table 7. After the strong CYP3A4 inhibitor or combined P-gp and strong CYP3A4 inhibitor have been discontinued for 3 to 5 elimination half-lives, the pralsetinib dose that was taken prior to the use of the inhibitor should be resumed. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDose modification for use with strong CYP3A4 inducers: Concomitant use of pralsetinib with strong CYP3A4 inducers should be avoided (see Precautions and Interactions). If concomitant use with a strong CYP3A4 inducer cannot be avoided, the dose of pralsetinib should be increased to double the current pralsetinib dose starting on Day 7 of co-administration of pralsetinib with the strong CYP3A4 inducer. After the strong CYP3A4 inducer has been discontinued for at least 14 days, the pralsetinib dose that was taken prior to the use of the inducer should be resumed.
Special populations: Renal impairment: No dose adjustment is recommended for patients with mild or moderate renal impairment (creatinine clearance [CLCR] 30 to 89 mL/min estimated by Cockcroft-Gault). Pralsetinib has not been studied in patients with severe renal impairment (CLCR 15 to 29 mL/min) or end-stage renal disease (CLCR <15 mL/min). Since pralsetinib elimination via the kidney is negligible, no dose adjustment is required in patients with severe renal impairment or end-stage renal disease (see PHARMACOLOGY: Pharmacokinetics under Actions).
Hepatic impairment: No dose adjustment is recommended for patients with mild hepatic impairment (total bilirubin ≤ upper limit of normal [ULN] and AST > ULN or total bilirubin > 1 to 1.5 times ULN and any AST). Pralsetinib has not been studied in patients with moderate or severe hepatic impairment, therefore its use in patients with moderate or severe hepatic impairment is not recommended (see PHARMACOLOGY: Pharmacokinetics under Actions).
Elderly: No dose adjustment is recommended for patients aged 65 years and above (see PHARMACOLOGY: Pharmacodynamics under Actions).
Paediatric population: NSCLC: The safety and efficacy of pralsetinib in paediatric patients below 18 years of age with RET fusion-positive advanced NSCLC have not been established. No data are available.
RET-Mutant Medullary Thyroid Cancer (MTC) and RET-Fusion Positive Thyroid Cancer: No dose adjustment of Gavreto is required in pediatric patients 12 years of age and older.
The safety and efficacy of Gavreto in pediatric patients under 12 years of age have not been established.
Method of administration: Gavreto is for oral use. Patients should swallow the hard capsules whole with a glass of water, on an empty stomach. They should not eat for at least two hours before and at least one hour after taking pralsetinib (see PHARMACOLOGY: Pharmacokinetics under Actions).