


 Sign Out
Sign Out

The most common grade 3/4 ADRs (reported at a frequency of ≥2%) in the pooled dataset for which the frequency for Kisqali plus any combination exceeds the frequency for placebo plus any combination were neutropenia, leukopenia, abnormal liver function tests, lymphopenia, infections, back pain, anaemia, fatigue, hypophosphataemia and vomiting.
Dose reduction due to adverse events, regardless of causality, occurred in 39.5% of patients receiving Kisqali in the phase III clinical studies regardless of the combination and permanent discontinuation was reported in 8.7% of patients receiving Kisqali and any combination in the phase III clinical studies.
In addition, the safety of Kisqali in combination with letrozole was evaluated in men (n=39) in an open-label, multicenter clinical study (COMPLEEMENT-1) for the treatment of patients with HR-positive, HER2-negative, advanced breast cancer who received no prior hormonal therapy for advanced disease. The median duration of exposure to Kisqali was 20.8 months (range: 0.5 to 30.6 months).
Adverse reactions occurring in men treated with Kisqali plus letrozole and goserelin or leuprolide were similar to those occurring in women treated with Kisqali plus endocrine therapy.
Tabulated list of adverse reactions: The overall safety evaluation of Kisqali is based on the pooled dataset from 1,065 patients who received Kisqali in combination with endocrine therapy (N=582 in combination with an aromatase inhibitor and N=483 in combination with fulvestrant) and who were included in the randomised, double-blind, placebo-controlled phase III clinical studies (MONALEESA-2, MONALEESA-7 NSAI subgroup and MONALEESA-3) in HR-positive, HER2-negative advanced or metastatic breast cancer.
Additional ADRs were identified post-marketing.
The median duration of exposure to study treatment across the pooled phase III studies dataset was 19.2 months, with 61.7% patients exposed ≥12 months.
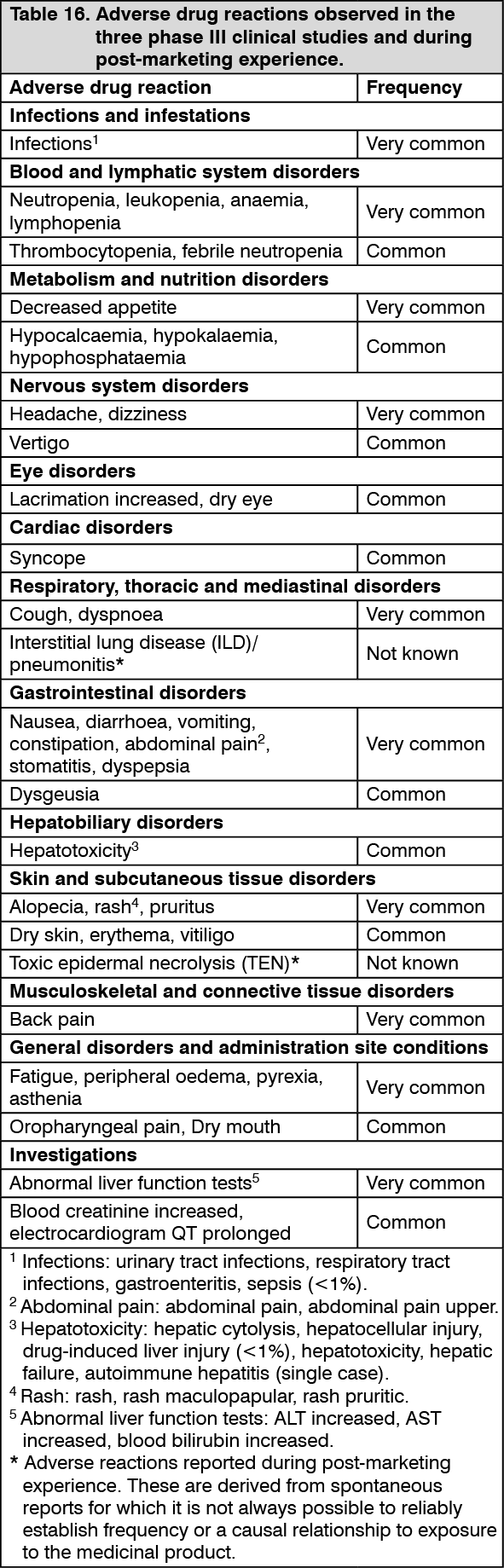
Adverse drug reactions from the phase III clinical studies (Table 16) are listed by MedDRA system organ class. Within each system organ class, the adverse drug reactions are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. In addition, the corresponding frequency category for each adverse drug reaction is based on the following convention (CIOMS III): very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); and not known (cannot be estimated from the available data). (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse drug reactions: Neutropenia: Neutropenia was the most frequently reported adverse drug reaction (75.4%) and a grade 3 or 4 decrease in neutrophil counts (based on laboratory findings) was reported in 62.0% of patients receiving Kisqali plus any combination in the phase III studies.
Among the patients who had grade 2, 3 or 4 neutropenia, the median time to onset was 17 days, for those patients who had an event. The median time to resolution of grade ≥3 (to normalisation or grade <3) was 12 days in the Kisqali plus any combination arms following treatment interruption and/or reduction and/or discontinuation. Febrile neutropenia was reported in about 1.7% of patients exposed to Kisqali in the phase III studies. Patients should be instructed to report any fever promptly.
Based on its severity, neutropenia was managed by laboratory monitoring, dose interruption and/or dose modification. Treatment discontinuation due to neutropenia was low (0.8%) (see Dosage & Administration and Precautions).
Hepatobiliary toxicity: In the phase III clinical studies, hepatobiliary toxicity events occurred in a higher proportion of patients in the Kisqali plus any combination arms compared with the placebo plus any combination arms (27.3% versus 19.6%, respectively), with more grade 3/4 adverse events reported in the patients treated with Kisqali plus any combination (13.2% versus 6.1%, respectively). Increases in transaminases were observed. Grade 3 or 4 increases in ALT (11.2% versus 1.7%) and AST (7.8% versus 2.1%) were reported in the Kisqali and placebo arms, respectively. Concurrent elevations in ALT or AST greater than three times the upper limit of normal and total bilirubin greater than two times the upper limit of normal, with normal alkaline phosphatase, in the absence of cholestasis occurred in 6 patients (4 patients in Study A2301 [MONALEESA-2], whose levels recovered to normal within 154 days and 2 patients in Study F2301 [MONALEESA-3], whose levels recovered to normal in 121 and 532 days, respectively, after discontinuation of Kisqali). There were no such cases reported in Study E2301 (MONALEESA-7).
Dose interruptions and/or adjustments due to hepatobiliary toxicity events were reported in 12.3% of Kisqali plus any combination treated patients, primarily due to ALT increased (7.9%) and/or AST increased (7.3%). Discontinuation of treatment with Kisqali plus any combination due to abnormal liver function tests or hepatotoxicity occurred in 2.4% and 0.3% of patients respectively (see Dosage & Administration and Precautions).
In the phase III clinical studies, 70.9% (90/127) of grade 3 or 4 ALT or AST elevation events occurred within the first 6 months of treatment. Among the patients who had grade 3 or 4 ALT/AST elevation, the median time to onset was 92 days for the Kisqali plus any combination arms. The median time to resolution (to normalisation or grade ≤2) was 21 days in the Kisqali plus any combination arms.
QT prolongation: In study E2301 (MONALEESA-7), the observed mean QTcF increase from baseline was approximately 10 msec higher in the tamoxifen plus placebo subgroup compared with the NSAI plus placebo subgroup, suggesting that tamoxifen alone had a QTcF prolongation effect which can contribute to the QTcF values observed in the Kisqali plus tamoxifen group. In the placebo arm, a QTcF interval increase of >60 msec from baseline occurred in 6/90 (6.7%) patients receiving tamoxifen and in no patients receiving a NSAI (see Pharmacology: Pharmacokinetics under Actions). A QTcF interval increase of >60 msec from baseline was observed in 14/87 (16.1%) patients receiving Kisqali plus tamoxifen and in 18/245 (7.3%) patients receiving Kisqali plus a NSAI. Kisqali is not recommended to be used in combination with tamoxifen (see Pharmacology: Pharmacodynamics under Actions).
In the phase III clinical studies 9.3% of patients in the Kisqali plus aromatase inhibitor or fulvestrant arms and 3.5% in the placebo plus aromatase inhibitor or fulvestrant arms had at least one event of QT interval prolongation (including ECG QT prolonged and syncope). Review of ECG data showed 15 patients (1.4%) had >500 msec post-baseline QTcF value, and 61 patients (5.8%) had a >60 msec increase from baseline in QTcF intervals. There were no reported cases of torsade de pointes. Dose interruptions/adjustments were reported in 2.9% of Kisqali plus aromatase inhibitor or fulvestrant treated patients due to electrocardiogram QT prolonged and syncope.
The analysis of ECG data showed 55 patients (5.2%) and 12 patients (1.5%) with at least one >480 msec post-baseline QTcF for the Kisqali plus aromatase inhibitor or fulvestrant arms and the placebo plus aromatase inhibitor or fulvestrant arms, respectively. Amongst the patients who had QTcF prolongation >480 msec, the median time to onset was 15 days regardless of the combination and these changes were reversible with dose interruption and/or dose reduction (see Dosage & Administration, Precautions and Pharmacology: Pharmacokinetics under Actions).
Patients with renal impairment: In the three pivotal studies, 341 patients with mild renal impairment and 97 patients with moderate renal impairment were treated with ribociclib. No patient with severe renal impairment was enrolled (see Pharmacology: Pharmacodynamics under Actions). There was a correlation between the degree of renal impairment at baseline and blood creatinine values during the treatment. Slightly increased rates of QT prolongation and thrombocytopenia were observed in patients with mild or moderate renal impairment. For monitoring and dose adjustment recommendations for these toxicities see Dosage & Administration and Precautions.
View ADR Monitoring Form