


 Sign Out
Sign Out

Posology: The recommended dose is 600 mg (three 200 mg film-coated tablets) of ribociclib once daily for 21 consecutive days followed by 7 days off treatment, resulting in a complete cycle of 28 days. The treatment should be continued as long as the patient is deriving clinical benefit from therapy or until unacceptable toxicity occurs.
Kisqali should be used together with 2.5 mg letrozole or another aromatase inhibitor or with 500 mg fulvestrant.
When Kisqali is used in combination with an aromatase inhibitor, the aromatase inhibitor should be taken orally once daily continuously throughout the 28-day cycle. Refer to the Summary of Product Characteristics (SmPC) of the aromatase inhibitor for additional details.
When Kisqali is used in combination with fulvestrant, fulvestrant is administered intramuscularly on days 1, 15 and 29, and once monthly thereafter. Refer to the SmPC of fulvestrant for additional details.
Treatment of pre- and perimenopausal women, or men, with the approved Kisqali combinations should also include an LHRH agonist in accordance with local clinical practice.
Kisqali can be taken with or without food (see Interactions). Patients should be encouraged to take their dose at approximately the same time each day, preferably in the morning. If the patient vomits after taking the dose or misses a dose, an additional dose should not be taken that day. The next prescribed dose should be taken at the usual time.
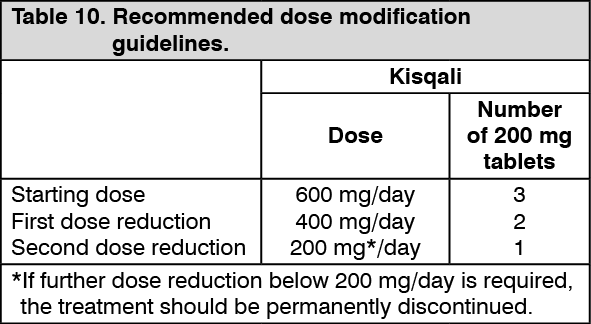
Dose modifications: Management of severe or intolerable adverse events (AEs) may require temporary dose interruption, reduction or discontinuation of Kisqali. If dose reduction is required, the recommended dose reduction guidelines are listed in Table 10. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTables 11, 12, 13, 14 and 15 summarise recommendations for dose interruption, reduction or discontinuation of Kisqali in the management of specific AEs. The clinical judgement of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment (see Precautions).
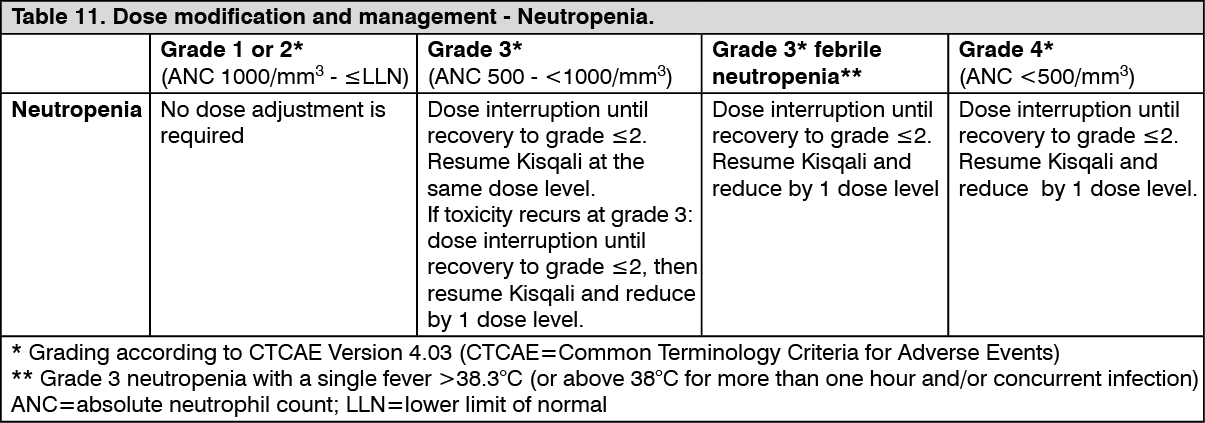
Complete blood counts (CBC) should be performed before initiating treatment with Kisqali. After initiating treatment CBC should be monitored every 2 weeks for the first 2 cycles, at the beginning of each of the subsequent 4 cycles, then as clinically indicated. (See Table 11.)
 Click on icon to see table/diagram/image
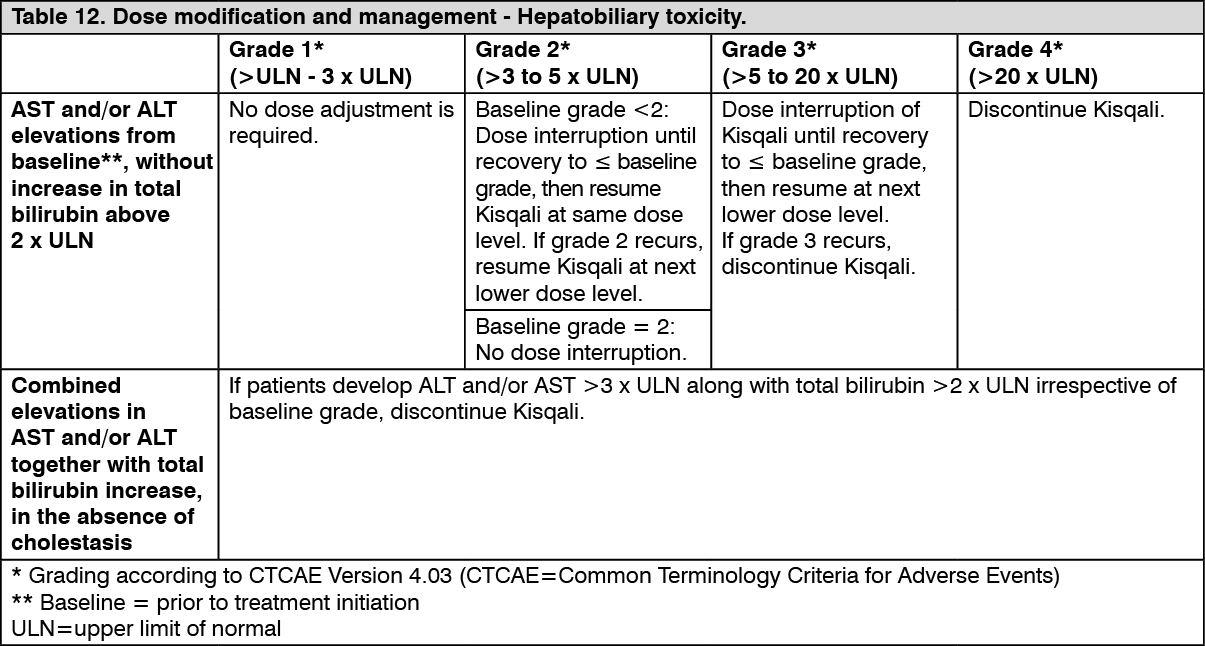
Click on icon to see table/diagram/imageLiver function tests (LFTs) should be performed before initiating treatment with Kisqali. After initiating treatment LFTs should be performed every 2 weeks for the first 2 cycles, at the beginning of each of the subsequent 4 cycles, then as clinically indicated. If grade ≥2 abnormalities are noted, more frequent monitoring is recommended. (See Table 12.)
 Click on icon to see table/diagram/image
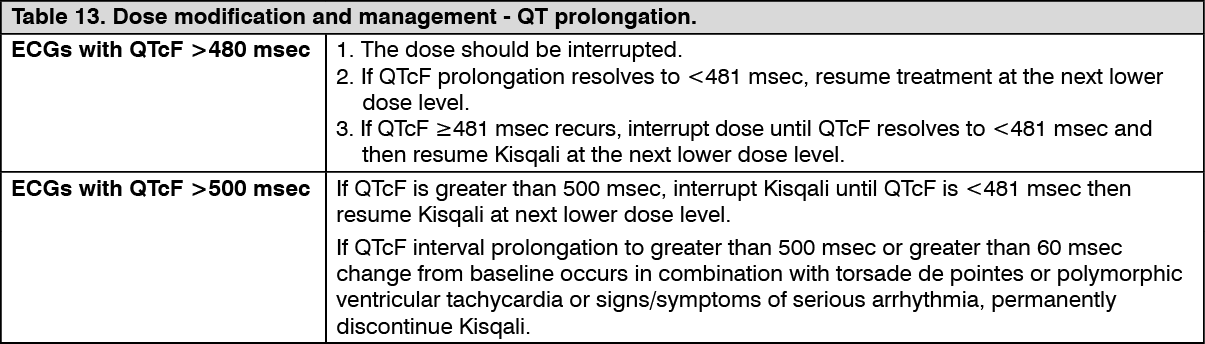
Click on icon to see table/diagram/imageECG should be assessed before initiating treatment with Kisqali. After initiating treatment, ECG should be repeated at approximately day 14 of the first cycle and at the beginning of the second cycle, then as clinically indicated. In case of QTcF prolongation during treatment, more frequent ECG monitoring is recommended. (See Tables 13, 14 and 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image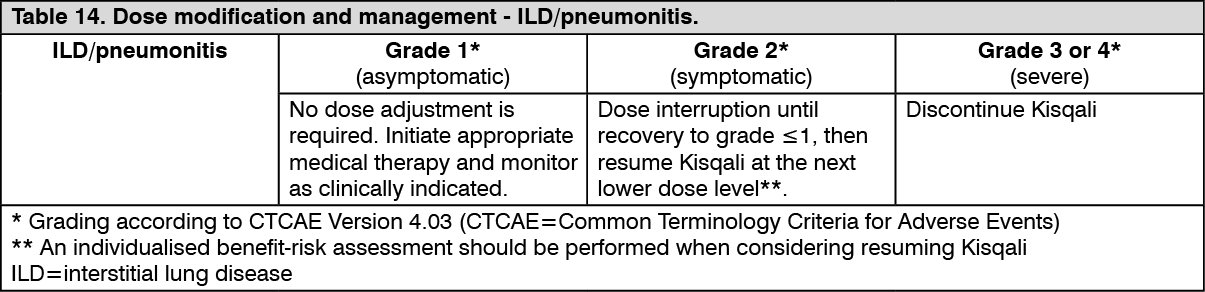 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image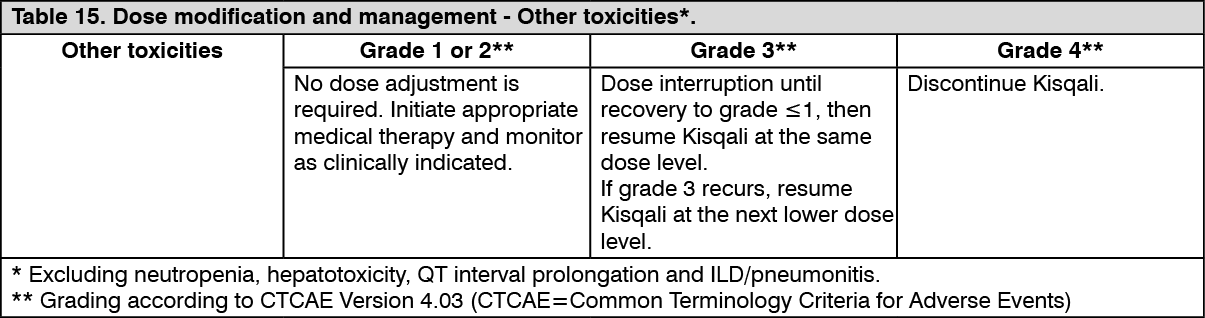 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRefer to the SmPC for the co-administered aromatase inhibitor, fulvestrant or LHRH agonist for dose modification guidelines and other relevant safety information in the event of toxicity.
Dose modification for use of Kisqali with strong CYP3A4 inhibitors: Concomitant use of strong CYP3A4 inhibitors should be avoided and an alternative concomitant medicinal product with less potential to inhibit CYP3A4 inhibition should be considered. If patients must be given a strong CYP3A4 inhibitor concomitantly with ribociclib, the Kisqali dose should be reduced to 400 mg once daily (see Interactions).
In patients who have had their dose reduced to 400 mg ribociclib daily and in whom initiation of co-administration of a strong CYP3A4 inhibitor cannot be avoided, the dose should be further reduced to 200 mg.
In patients who have had their dose reduced to 200 mg ribociclib daily and in whom initiation of co-administration of a strong CYP3A4 inhibitor cannot be avoided, Kisqali treatment should be interrupted.
Due to inter-patient variability, the recommended dose adjustments may not be optimal in all patients, therefore close monitoring of signs of toxicity is recommended. If the strong inhibitor is discontinued, the Kisqali dose should be changed to the dose used prior to the initiation of the strong CYP3A4 inhibitor after at least 5 half-lives of the strong CYP3A4 inhibitor (see Precautions, Interactions and Pharmacology: Pharmacokinetics under Actions).
Special populations: Renal impairment: No dose adjustment is necessary in patients with mild or moderate renal impairment. A starting dose of 200 mg is recommended in patients with severe renal impairment. Kisqali has not been studied in breast cancer patients with severe renal impairment (see Precautions, Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
Hepatic impairment: No dose adjustment is necessary in patients with mild hepatic impairment (Child-Pugh class A). Patients with moderate (Child-Pugh class B) and severe hepatic impairment (Child-Pugh class C) can have increased (less than 2-fold) exposure to ribociclib and the starting dose of 400 mg Kisqali once daily is recommended (see Pharmacology: Pharmacokinetics under Actions).
Paediatric population: The safety and efficacy of Kisqali in children and adolescents aged below 18 years have not been established. No data are available.
Elderly: No dose adjustment is required in patients over 65 years of age (see Pharmacology: Pharmacokinetics under Actions).
Method of administration: Kisqali should be taken orally once daily with or without food. The tablets should be swallowed whole and should not be chewed, crushed or split prior to swallowing. No tablet should be ingested if it is broken, cracked or otherwise not intact.