


 Sign Out
Sign Out


Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety data described in this section reflect exposure to BLINCYTO in clinical trials in which 282 patients (212 adult and 70 pediatric patients) with relapsed or refractory ALL were treated with a recommended dose and schedule. All patients received at least one dose of BLINCYTO. The most common adverse reactions (≥ 20%) in the safety population were pyrexia, headache, nausea, edema, hypokalemia, anemia, febrile neutropenia, neutropenia, thrombocytopenia, and abdominal pain. For some adverse reactions, there were differences in incidence rates by age subgroup (see Use in Specific Populations under Precautions).
The safety population included 225 patients weighing 45 kg or more and 57 patients weighing less than 45 kg. In general, the adverse reactions in the BLINCYTO-treated patients less than 45 kg were similar in type to those seen in patients greater than or equal to 45 kg.
Patients Greater Than or Equal to 45 kg: The median age of patients greater than or equal to 45 kg was 34 years (range: 11 to 79 years), 63% were male, 79% were White, 3% were Asian, and 3% were Black or African American.
Serious adverse reactions were reported in 61% of patients. The most common serious adverse reactions (≥ 2%) included febrile neutropenia, pyrexia, sepsis, pneumonia, device-related infection, neutropenia, tremor, overdose, encephalopathy, infection, confusion, and headache. Adverse reactions of grade 3 or higher were reported in 80% of patients. Discontinuation of therapy due to adverse reactions occurred in 16% of patients treated with BLINCYTO. The adverse reactions reported most frequently as the reason for discontinuation of treatment included encephalopathy and sepsis. Fatal adverse events occurred in 12% of patients. The majority of the fatal events were infections. No fatal adverse events occurred on treatment among patients in remission.
Patients Less Than 45 kg: The median age of patients less than 45 kg was 6 years (range: 7 months to 64 years), 68% were male, and 77% were White.
Serious adverse reactions were reported in 51% of patients. The most common serious adverse reactions (≥ 2%) included pyrexia, febrile neutropenia, cytokine release syndrome, convulsion, device-related infection, hypoxia, sepsis, and overdose. Adverse reactions of Grade 3 or higher were reported in 88% of patients. Discontinuation of therapy due to adverse reactions occurred in 5% of patients treated with BLINCYTO. Adverse reactions that led to discontinuation of treatment were CRS and fungal infection.
Three patients experienced a fatal adverse event within 30 days of the last dose of BLINCYTO (2 infection and 1 multi-organ failure after undergoing subsequent HSCT).
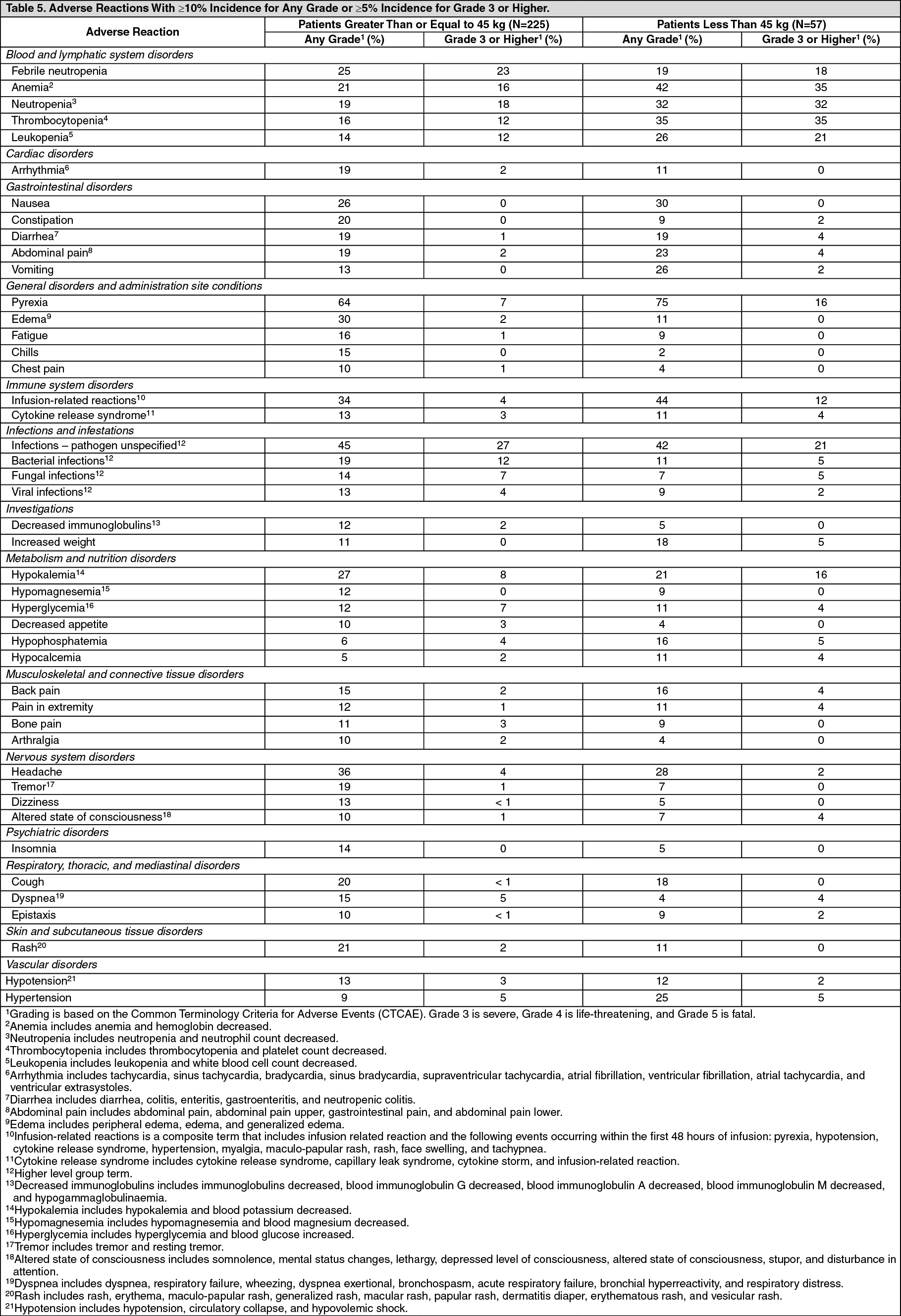
The adverse reactions with ≥ 10% incidence for any grade or ≥ 5% incidence for Grade 3 or higher are summarized in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor patients weighing greater than or equal to 45 kg and patients less than 45 kg, additional important adverse reactions that did not meet the threshold criteria for inclusion in Table 5 were, in each weight cohort respectively: leukocytosis (2%, 4%), lymphopenia (1%, 2%), increased gamma-glutamyl-transferase (6%, 2%), tumor lysis syndrome (4%, 0%), hypoalbuminemia (4%, 7%), encephalopathy (5%, 2%), paresthesia (5%, 2%), aphasia (4%, 0%), convulsion (2%, 4%), memory impairment (2%, 0%), cognitive disorder (1%, 0%), speech disorder (< 1%, 0%), confusional state (7%, 0%), and disorientation (3%, 0%), respectively.
Hypersensitivity reactions related to BLINCYTO treatment were hypersensitivity (1%) and bronchospasm (< 1%).
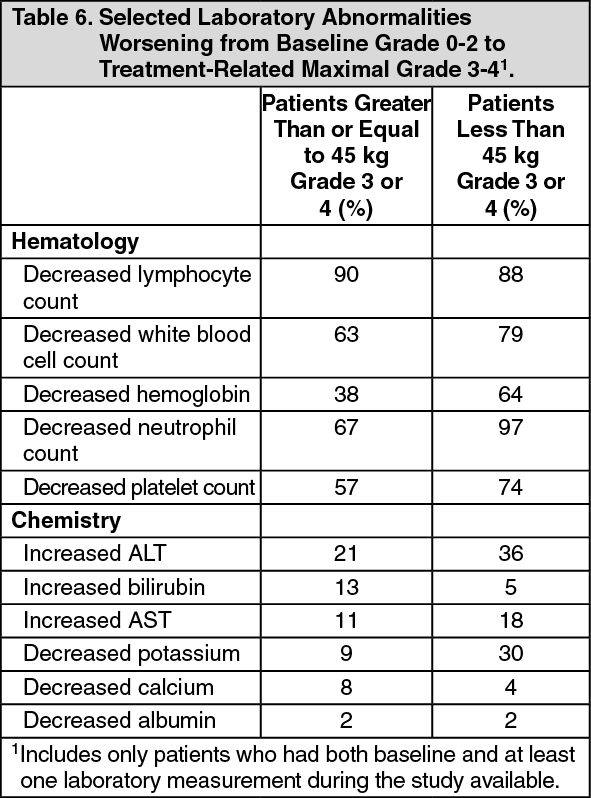
Selected laboratory abnormalities worsening from baseline Grade 0-2 to treatment-related maximal Grade 3-4 are shown in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePostmarketing Experience: The following adverse reactions have been identified during postapproval use of BLINCYTO. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Fatal pancreatitis, has been reported in patients receiving BLINCYTO in combination with dexamethasone (see Precautions).
Immunogenicity: As with all therapeutic proteins, there is potential for immunogenicity. The immunogenicity of BLINCYTO has been evaluated using either an electrochemiluminescence detection technology (ECL) or an enzyme-linked immunosorbent assay (ELISA) screening immunoassay for the detection of binding anti-blinatumomab antibodies. For patients whose sera tested positive in the screening immunoassay, an in vitro biological assay was performed to detect neutralizing antibodies.
In clinical studies, less than 1% of patients treated with BLINCYTO tested positive for binding anti-blinatumomab antibodies. All patients who tested positive for binding antibodies also tested positive for neutralizing anti-blinatumomab antibodies. Anti-blinatumomab antibody formation may affect pharmacokinetics of BLINCYTO.
The detection of anti-blinatumomab antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to blinatumomab with the incidence of antibodies to other products may be misleading.
View ADR Monitoring Form