Pharmacology: Pharmacodynamics: During the continuous intravenous infusion over 4 weeks, the pharmacodynamic response was characterized by T-cell activation and initial redistribution, reduction in peripheral B cells, and transient cytokine elevation.
Peripheral T cell redistribution (ie, T cell adhesion to blood vessel endothelium and/or transmigration into tissue) occurred after start of BLINCYTO infusion or dose escalation. T cell counts initially declined within 1 to 2 days and then returned to baseline levels within 7 to 14 days in majority of patients. Increase of T cell counts above baseline (T cell expansion) was observed in few patients.
Peripheral B cell counts decreased to less than or equal to 10 cells/microliter during the first treatment cycle at doses ≥ 5 mcg/m
2/day or ≥ 9 mcg/day in the majority of patients. No recovery of peripheral B-cell counts was observed during the 2-week BLINCYTO-free period between treatment cycles. Incomplete depletion of B cells occurred at doses of 0.5 mcg/m
2/day and 1.5 mcg/m
2/day and in a few patients at higher doses.
Cytokines including IL-2, IL-4, IL-6, IL-8, IL-10, IL-12, TNF-α, and IFN-γ were measured, and IL-6, IL-10, and IFN-γ were elevated. The highest elevation of cytokines was observed in the first 2 days following start of BLINCYTO infusion. The elevated cytokine levels returned to baseline within 24 to 48 hours during the infusion. In subsequent treatment cycles, cytokine elevation occurred in fewer patients with lesser intensity compared to the initial 48 hours of the first treatment cycle.
Mechanism of Action: Blinatumomab is a bispecific CD19-directed CD3 T-cell engager that binds to CD19 expressed on the surface of cells of B-lineage origin and CD3 expressed on the surface of T cells. It activates endogenous T cells by connecting CD3 in the T-cell receptor (TCR) complex with CD19 on benign and malignant B cells. Blinatumomab mediates the formation of a synapse between the T-cell and the tumor cell, upregulation of cell adhesion molecules, production of cytolytic proteins, release of inflammatory cytokines, and proliferation of T cells, which result in redirected lysis of CD19+ cells.
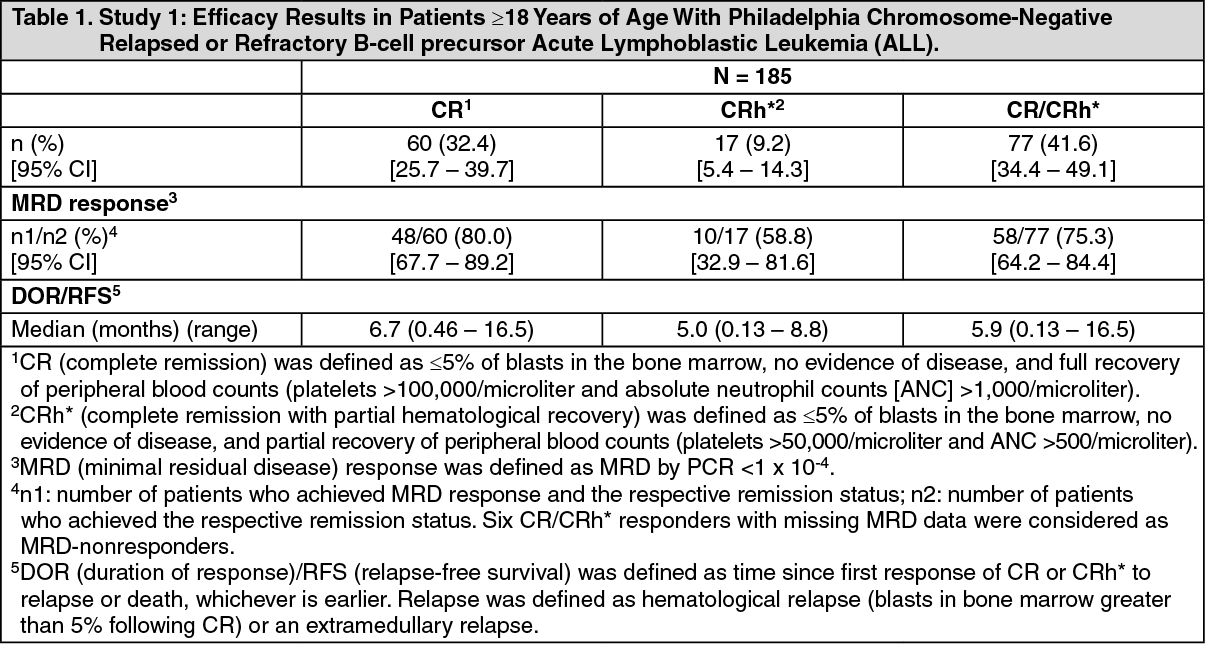
Clinical Studies: Relapsed/Refractory Acute Lymphoblastic Leukemia: Study 1: Study 1 was an open-label, multicenter, single-arm study. Eligible patients were ≥ 18 years of age with Philadelphia chromosome-negative relapsed or refractory B-cell precursor ALL (relapsed with first remission duration of ≤ 12 months in first salvage or relapsed or refractory after first salvage therapy or relapsed within 12 months of allogeneic hematopoietic stem cell transplantation [HSCT], and had ≥ 10% blasts in bone marrow).
BLINCYTO was administered as a continuous intravenous infusion. The recommended dose for this study was determined to be 9 mcg/day on Days 1-7 and 28 mcg/day on Days 8-28 for Cycle 1, and 28 mcg/day on Days 1-28 for subsequent cycles. Dose adjustment was possible in case of adverse events. The treated population included 185 patients who received at least 1 infusion of BLINCYTO; the median number of treatment cycles was 2 (range: 1 to 5). Patients who responded to BLINCYTO but later relapsed had the option to be retreated with BLINCYTO. Among treated patients, the median age was 39 years (range: 18 to 79 years), 63 out of 185 (34.1%) had undergone HSCT prior to receiving BLINCYTO, and 32 out of 185 (17.3%) had received more than 2 prior salvage therapies.
Efficacy was based on the complete remission (CR) rate, duration of CR, and proportion of patients with an MRD-negative CR/CR with partial hematological recovery (CR/CRh*) within 2 cycles of treatment with BLINCYTO. Seventy-seven out of 185 (41.6%) evaluable patients achieved CR/CRh* within the first 2 treatment cycles, with the majority of responses (81%, 62 out of 77) occurring within Cycle 1 of treatment. See Table 1 for efficacy results from this study. The HSCT rate among those who achieved CR/CRh* was 39% (30 out of 77). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Study 2: Study 2 was an open-label, multicenter, single-arm study in pediatric patients with relapsed or refractory B-cell precursor ALL (second or later bone marrow relapse, any marrow relapse after allogeneic HSCT, or refractory to other treatments, and had > 25% blasts in bone marrow). BLINCYTO was administered at 5 mcg/m
2/day on Days 1-7 and 15 mcg/m
2/day on Days 8-28 for cycle 1, and 15 mcg/m
2/day on Days 1-28 for subsequent cycles. Dose adjustment was possible in case of adverse events. Patients who responded to BLINCYTO but later relapsed had the option to be retreated with BLINCYTO.
Among the 70 treated patients, the median age was 8 years (range: 7 months to 17 years), 40 out of 70 (57.1%) had undergone allogeneic HSCT prior to receiving BLINCYTO, and 39 out of 70 (55.7%) had refractory disease. The median number of treatment cycles was 1 (range: 1 to 5).
Twenty-three out of 70 (32.9%) patients achieved CR/CRh* within the first 2 treatment cycles with 17 out of 23 (73.9%) occurring within cycle 1 of treatment. See Table 2 for the efficacy results from the study. The HSCT rate among those who achieved CR/CRh* was 48% (11 out of 23). (See Table 2.)
Click on icon to see table/diagram/image
Pharmacokinetics: The pharmacokinetics of blinatumomab appear linear over a dose range from 5 to 90 mcg/m
2/day (approximately equivalent to 9 to 162 mcg/day) in adult patients. Following continuous intravenous infusion, the steady-state serum concentration (C
ss) was achieved within a day and remained stable over time. The increase in mean C
ss values was approximately proportional to the dose in the range tested. At the clinical doses of 9 mcg/day and 28 mcg/day for the treatment of relapsed/refractory ALL, the mean (SD) C
ss was 211 (258) pg/mL and 621 (502) pg/mL, respectively.
Distribution: The estimated mean (SD) volume of distribution based on terminal phase (Vz) was 4.52 (2.89) L with continuous intravenous infusion of blinatumomab.
Metabolism: The metabolic pathway of blinatumomab has not been characterized. Like other protein therapeutics, BLINCYTO is expected to be degraded into small peptides and amino acids via catabolic pathways.
Elimination: The estimated mean (SD) systemic clearance with continuous intravenous infusion in patients receiving blinatumomab in clinical studies was 2.92 (2.83) L/hour. The mean (SD) half-life was 2.11 (1.42) hours. Negligible amounts of blinatumomab were excreted in the urine at the tested clinical doses.
Gender, Age, and Body Surface Area: Results of population pharmacokinetic analyses indicate that age (0.62 to 80 years of age) and gender do not influence the pharmacokinetics of blinatumomab. Body surface area (0.37 to 2.70 m
2) influences the pharmacokinetics of blinatumomab, however the clinical relevance of this effect is unknown.
Hepatic Impairment: No formal pharmacokinetic studies using BLINCYTO have been conducted in patients with hepatic impairment.
Renal Impairment: No formal pharmacokinetic studies of blinatumomab have been conducted in patients with renal impairment.
Pharmacokinetic analyses showed an approximately 2-fold difference in mean blinatumomab clearance values between patients with moderate renal impairment (CrCL ranging from 30 to 59 mL/min, N = 21) and normal renal function (CrCL more than 90 mL/min, N = 215). However, high interpatient variability was discerned (CV% up to 95.6%), and clearance values in renal impaired patients were essentially within the range observed in patients with normal renal function. There is no information available in patients with severe renal impairment (CrCL less than 30 mL/min) or patients on hemodialysis.
Drug Interactions: Transient elevation of cytokines may suppress CYP450 enzyme activities (see Interactions and Pharmacodynamics).
Specific Populations: Pediatrics: The pharmacokinetics of blinatumomab appear linear over a dose range from 5 to 30 mcg/m
2/day in pediatric patients. At the recommended doses, the mean (SD) steady state concentration (C
ss) values were 162 (179) and 533 (392) pg/mL at 5 and 15 mcg/m
2/day doses, respectively. The estimated mean (SD) volume of distribution (V
z), clearance (CL) and terminal half-life (t
1/2,z) were 3.91 (3.36) L/m
2, 1.88 (1.90) L/hour/m
2 and 2.19 (1.53) hours, respectively.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: No carcinogenicity or genotoxicity studies have been conducted with blinatumomab.
No studies have been conducted to evaluate the effects of blinatumomab on fertility. A murine surrogate molecule had no adverse effects on male and female reproductive organs in a 13-week repeat-dose toxicity study in mice.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image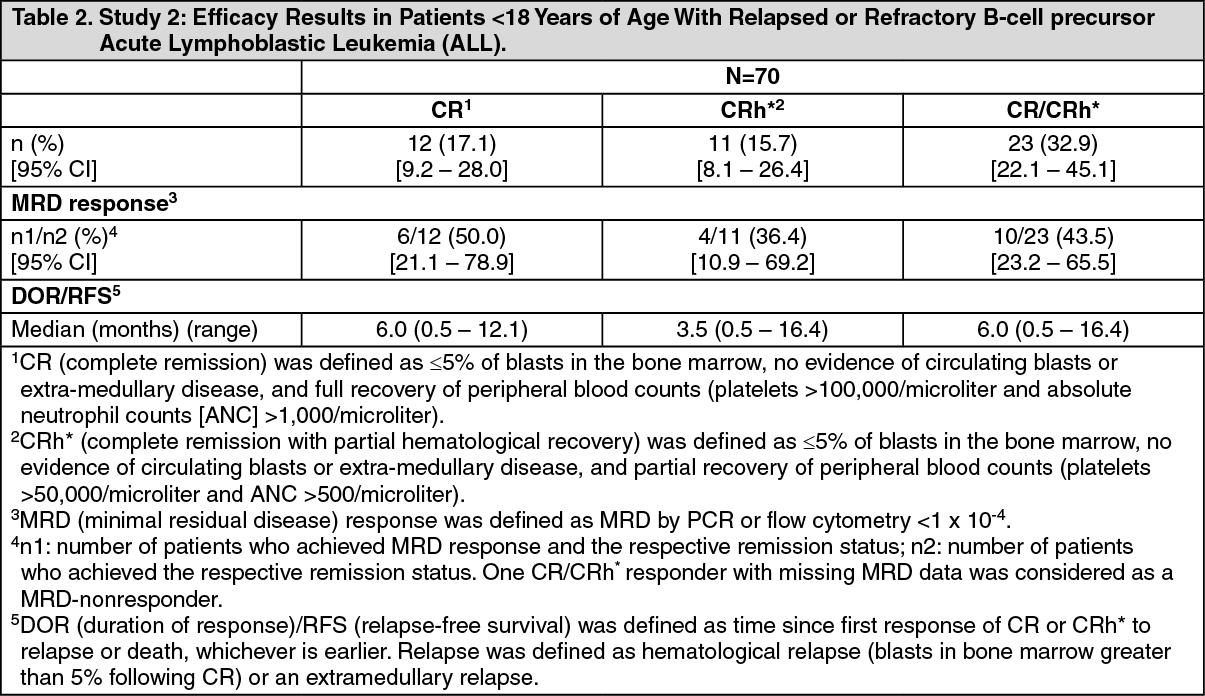 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image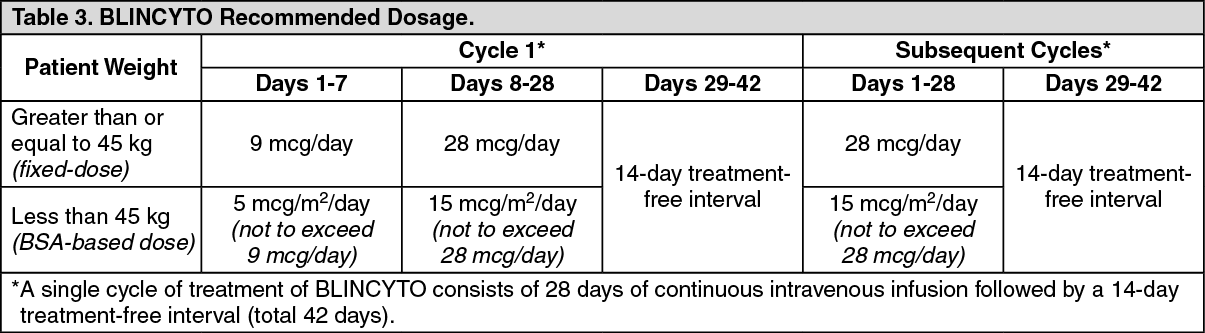 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
