Pharmacology: Pharmacodynamics: Mechanism of Action: Clindamycin: Clindamycin is a lincosamide antibiotic with bacteriostatic action against gram-positive aerobes and a wide range of anaerobic bacteria. Lincosamides such as clindamycin bind to the 50S ribosomal subunit of susceptible bacteria and prevent elongation of peptide chains by interfering with peptidyl transfer, thereby suppressing protein synthesis. The action of clindamycin is predominantly bacteriostatic although high concentrations may be slowly bactericidal against sensitive strains. Clindamycin phosphate is inactive
in vitro, and is hydrolysed
in vivo to active clindamycin.
Benzoyl Peroxide: Benzoyl peroxide is a higly lipophilic oxidizing agent with bactericidal and mild keratolytic effects. It contributes a nonspecific bactericidal mechanism (the formation of reactive oxygen species) to the combination therapy and thereby suppresses the emergence of drug resistance organisms.
Pharmacodynamic Effects: Clindamycin: Clindamycin has been shown to have
in vitro activity against
Propionibacterium acnes, an organism that has been associated with
acne vulgaris.
P. acnes resistance to clindamycin has been documented. Clindamycin
in vitro inhibits
P. acnes [minimum inhibitory concentration (MIC) 0.4 mcg/mL]. Free fatty acids on the skin surface have been decreased from approximately 14% to 2% following application of clindamycin. It also reduces inflammation by inhibiting leukocyte chemotaxis.
Benzoyl Peroxide: The effectiveness of benzoyl peroxide in the treatment of acne vulgaris is primarily attributable to its bactericidal activity, especially with respect to
P. acnes. The bactericidal activity of benzoyl peroxide is due to the release of active or free radical oxygen capable of oxidizing bacterial proteins. Benzoyl peroxide is also believed to be effective in the treatment of acne on account of its anti-inflammatory and mild keratolytic properties.
Resistance and Cross-Resistance: The treatment of acne with topical and oral antibiotics used as monotherapy such as clindamycin and erythromycin has been associated with the development of antimicrobial resistance in
P. acnes as well as commensal flora (eg,
Staphylococcus aureus, Streptococcus pyogenes). The use of clindamycin may result in developing inducible resistance in these organisms. Benzoyl peroxide has a bactericidal effect and it has not been shown to induce emergence resistance in
P. acnes. The inclusion of benzoyl peroxide in Duac has shown to reduce clindamycin resistant
P. acne counts (see Precautions). This has not been studied with clindamycin 1%/benzoyl peroxide 3%.The prevalence of acquired resistance may vary geographically and over time for selected organisms. Local information of resistance is desirable, particularly when treating severe infections.
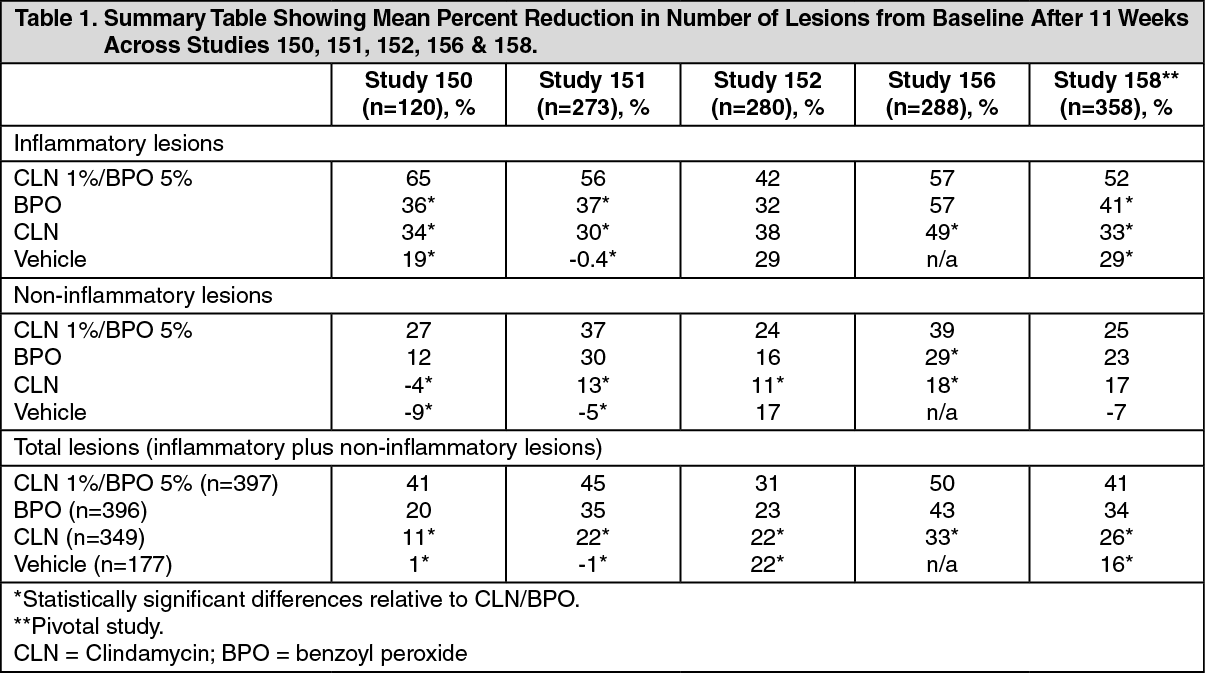
Clinical Studies: The safety and efficacy of Duac were evaluated in 5 randomised double-blind clinical studies of 1319 patients with facial acne vulgaris with both inflammatory and noninflammatory lesions. Treatment was applied once daily for 11 weeks and patients were evaluated and lesions counted 2, 5, 8, and 11 weeks. The mean percentage reduction in the number of all lesions after 11 weeks is shown in Table 1. (See Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The mean percentage reduction in total lesions was significantly greater with Duac than clindamycin or vehicle in all 5 studies. The observed improvement was consistently greater with this drug than benzoyl peroxide alone, but the difference did not achieve statistical significance in all individual studies.
Against inflammatory lesions, Duac was significantly superior to clindamycin alone in 4 of 5 studies and to benzoyl peroxide alone in 3 of 5 studies. Against noninflammatory lesions, this drug was significantly superior to clindamycin alone in 4 of 5 studies.
Overall improvement in acne was assessed by the physician and was significantly superior with Duac than with either benzoyl peroxide or clindamycin alone in 3 of 5 studies. An effect on inflammatory lesions was apparent from week 2 of treatment. The effect on noninflammatory lesions was more variable, with efficacy generally apparent after 2-5 weeks of treatment.
Pharmacokinetics: Absorption/Distribution/Metabolism: Clindamycin: Clindamycin phosphate is rapidly hydrolyzed to clindamycin by skin phosphatases. Clindamycin is further metabolized to clindamycin sulfoxide. Significant levels of clindamycin have been detected in comedones of patients who have applied topical clindamycin phosphate for 2 weeks. There is no evidence that the skin acts as a reservoir for clindamycin after repeated applications or that it accumulates systematically. Clindamycin is metabolized in the liver to active and inactive metabolites.
Benzoyl Peroxide: Benzyl peroxide is absorbed in the skin where it is metabolised to benzoic acid. Following topical application, <5% of the dose enters systemic circulation as benzoic acid.
A comparative study of the pharmacokinetics of Duac gel (1 g applied to the face once daily) and 1% clindamycin solution (0.5 g applied to the face twice daily) in 78 patients with moderate to severe acne indicated that mean plasma clindamycin levels during the 4-week dosing period were very low (<0.5 ng/mL) for both treatment groups. The presence of benzoyl peroxide in the formulation did not have an effect on the percutaneous absorption of clindamycin. In an open-label study of patients with moderate to severe acne vulgaris, approximately 4 g of Duac gel was applied once daily for 5 days to the face, upper chest, and upper back and shoulders. Two formulations were studied (24 patients in each group), one containing methylparaben and the other was preservative-free. Clindamycin was slowly absorbed after topical application, reaching maximal observed plasma concentrations within 6-8 hrs. Geometric mean maximal plasma clindamycin exposure (C
max and AUC
0-∞) on day 5 was 1.095 ng/mL and 16.3 ng·h/mL, respectively, in the methylparaben formulation and 0.806 ng/mL and 11.4 ng·h/mL, respectively, in the preservative-free formulation. Systemic exposure to clindamycin sulfoxide was lower relative to clindamycin, as mean C
max and AUC values were approximately 4- to 5-fold higher on average for clindamycin compared with clindamycin sulfoxide. This ratio was comparable across all formulations, indicating that the conversion of clindamycin to its metabolite is not affected by formulation.
Elimination: Clindamycin: Clindamycin has an elimination t
½ of approximately 9 hrs and is excreted mainly in the urine as the parent compound. Following multiple topical applications of clindamycin gel, <0.06% of the total dose was excreted in the urine.
Benzoyl Peroxide: Benzoyl peroxide is excreted as benzoic acid in the urine.
Clindamycin/benzoyl peroxide gel: A comparative study of the pharmacokinetics of Duac gel (1 g applied to the face once daily) and 1% clindamycin solution (0.5 g applied to the face twice daily) in 78 patients for 4 weeks, indicated no statistically significant differences in the amounts of clindamycin and clindamycin sulfoxide excreted in the 24-hr period after the last dose were detected between treatments.
Special Patient Populations: Children: Not relevant for this product.
Elderly: See Dosage & Administration.
Renal Impairment: See Dosage & Administration.
Hepatic Impairment: See Dosage & Administration.
Toxicology: Nonclinical Information: Carcinogenesis/Mutagenesis: No genotoxicity or mutagenicity studies have been conducted with topical clindamycin/benzoyl peroxide gel.
Clindamycin: Clindamycin phosphate was not genotoxic in
Salmonella typhimurium, a chromosome aberration assay or in a rat micronucleus test.
Benzoyl Peroxide: Both the carcinogenicity and photocarcinogenicity of benzoyl peroxide have been extensively assessed in both mice and hamsters, by various routes of administration, in studies ranging from 42-100 weeks in duration. The overall conclusion is that benzoyl peroxide is considered to be neither carcinogenic nor photocarcinogenic in topical acne products at a concentration of 2.5-10%.
The genotoxicity of benzoyl peroxide was extensively assessed
in vitro and
in vivo. While in a few
in vitro studies benzoyl peroxide showed weak mutagenicity, the overall genotoxicity profile did not indicate significant biological relevance.
Clindamycin/Benzoyl Peroxide Gel: In a 2-year carcinogenicity study in mice, topical administration of clindamycin 1%/benzoyl peroxide 5% gel at dose levels up to 8000 mg/kg/day (24,000 mg/m
2/day) showed no evidence of increased carcinogenic risk, compared with controls.
In a 52-week photococarcinogenicity study in which hairless mice were exposed to both ultraviolet radiation and clindamycin 1%/benzoyl peroxide 5% gel at dose levels up to 2500 mg/kg/day (7500 mg/m
2/day), a slight reduction in the median time to onset of tumors was observed, as compared to ultraviolet radiation alone.
Reproductive Toxicology: Fertility and Pregnancy: No fertility studies were conducted with topical clindamycin/benzoyl peroxide gel.
Clindamycin: Fertility studies in rats treated orally with up to 300 mg/kg/day of clindamycin revealed no effects on fertility or mating ability.
Reproduction studies have been performed in rats and mice using SC and oral doses of clindamycin phosphate, clindamycin hydrochloride and clindamycin palmitate. These studies revealed no evidence of fetal harm.
The highest dose used in the rat and mouse teratogenicity studies was equivalent to a clindamycin phosphate dose of 432 mg/kg. For a rat, that dose is 84-fold higher, and for a mouse 42-fold higher, than the anticipated human dose of clindamycin phosphate from 1% clindamycin phosphate foam based on a mg/m
2 comparison.
Benzoyl Peroxide: In a combined repeat dose and reproduction/development toxicity study, benzoyl peroxide (250, 500, or 1000 mg/kg/day) was administered orally to male rats for 29 days and female rats for 41-51 days. There were no treatment-related changes observed in the mating period, mating rate, conception rate, delivery rate, birth rate, pregnancy period, luteinisation number, implantation number and the rate of losing embryos and fetuses after implantation. In pups, body weight was significantly decreased in the high-dose group. The no-observed-adverse-effect level (NOAEL) for reproductive toxicities was considered to be 500 mg/kg/day.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out