


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Levofloxacin is a synthetic antibacterial agent from fluoroquinolone group and is S-enantiomer of racemic mixture of medicinal product ofloxacin.
Mechanism of action: As an antibacterial agent from fluoroquinolone group, levofloxacin has effect on complex of DNA-DNA-gyrase and topoisomerase IV.
Pharmacokinetics/pharmacodynamics ratio: Level of bacterial activity of levofloxacin depends on ratio of peak serum concentration (Сmах) or area under pharmacokinetics curve (AUC) and minimum inhibitory concentration (MIC).
Mechanism of resistance: Main mechanism of resistance is a result of mutation in genes of gyr-A. In vitro there is cross resistance between levofloxacin and other fluoroquinolones. Due to mechanism of action, there is no cross resistance between levofloxacin and other classes of antibacterial agents.
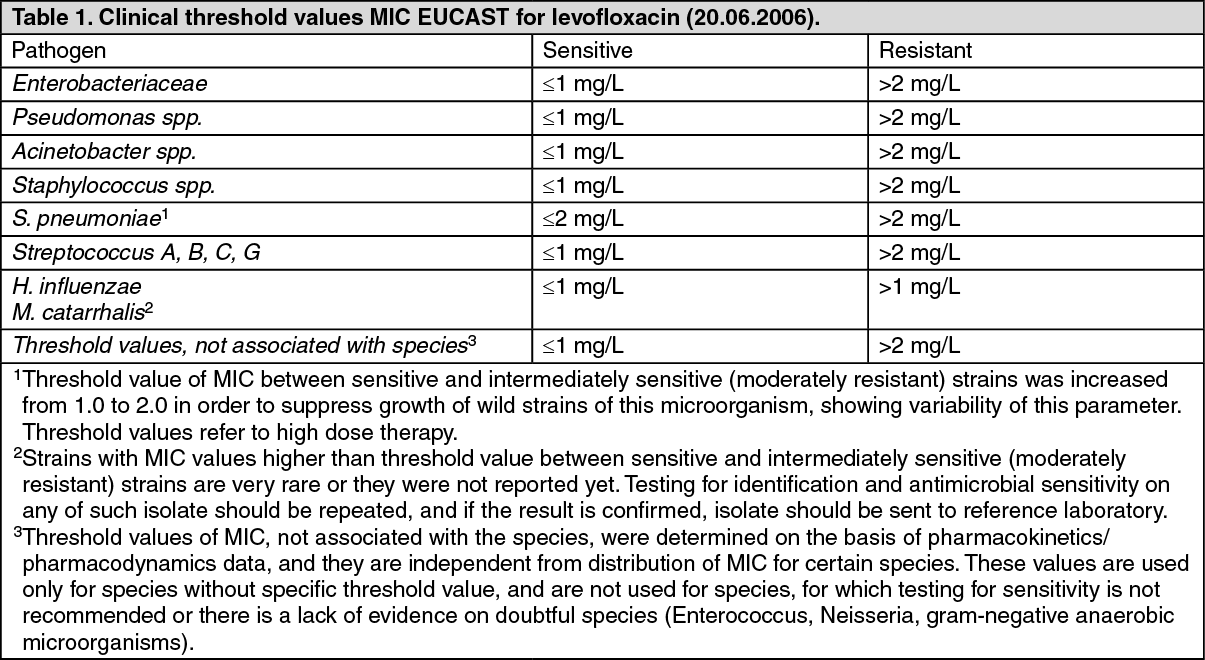
Threshold values: Recommended by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) threshold values of MIC for levofloxacin, that separate sensitive microorganisms from organisms intermediately sensitive to (moderately resistant) and intermediately sensitive from resistant organisms, are given in a table of MIC testing (mg/l) as follows. (See Table 1.)
 Click on icon to see table/diagram/image
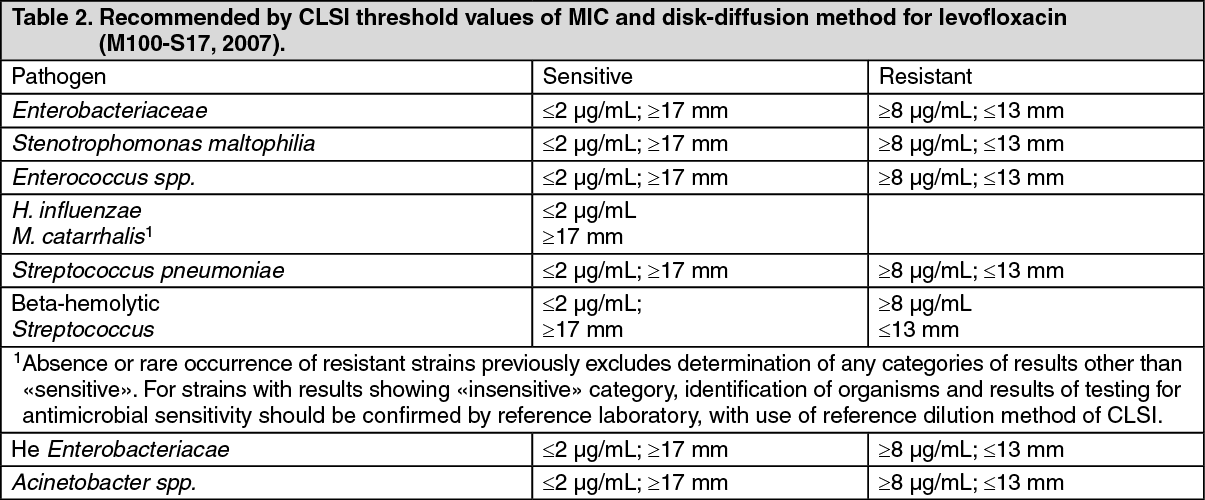
Click on icon to see table/diagram/imageRecommended by СLSІ (Clinical and Laboratory Standards Institute, earlier-NCCLS) threshold values of MIC for levofloxacin, that separate sensitive organisms from intermediately sensitive ones, and intermediately sensitive from resistant organisms, are specified in table as follows, for MIC testing (μg/mL) or disk-diffusion method (diameter of zone [mm] with the use of disk with levofloxacin is 5 μg). (See Table 2.)
 Click on icon to see table/diagram/image
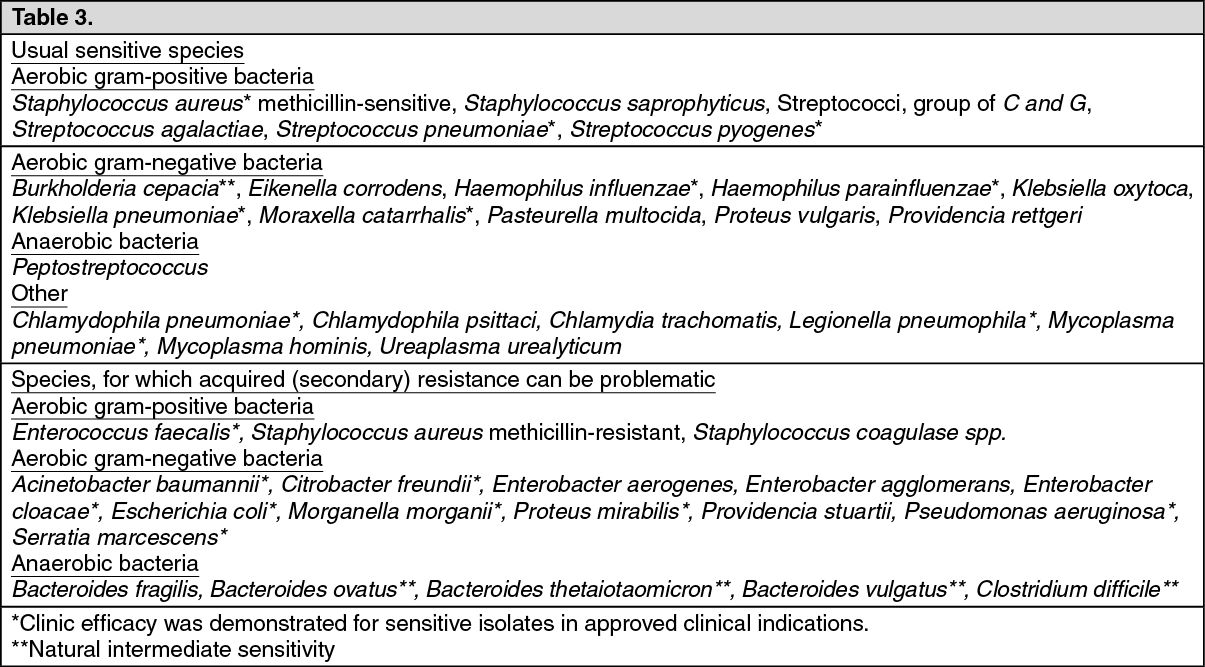
Click on icon to see table/diagram/imageAntibacterial spectrum: Spreading of resistance could vary geographically and in course of time, for selected species, and it is advisable to obtain local information concerning resistance, especially for treatment of severe infections. If necessary, a patient should consult a professional, when local occurrence of resistance is such one, that drug utility at least at certain kinds of infections is questionable. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther data: Hospital acquired infections caused by Р. aeruginosa could require combined therapy.
Pharmacokinetics: Absorption: There is no significant difference in pharmacokinetics of levofloxacin after intravenous and oral administration.
After intravenous administration, drug is accumulated in mucosa of bronchi and bronchial mucous of lung tissue (lung concentration exceeds the one in blood plasma), urine. Levofloxacin penetrates badly into cerebrospinal liquid.
Distribution: Approximately 30-40% of levofloxacin is bound with serum protein. Cumulative effect of levofloxacin at the use of 500 mg once a day multidose administration is practically absent. There is insignificant, but predictable cumulative effect after use of doses of 500 mg twice a day. Steady state is achieved during 3 days.
Penetration into body tissues and fluids: Penetration into mucosa of bronchi, bronchial mucous of lung tissues (BMLT): Maximum concentrations of levofloxacin in mucosa of bronchi and lung bronchial mucous after use of 500 mg orally were 8.3 μg/g and 10.8 μg/mL respectively. These parameters were achieved within one hour after drug administration.
Penetration into lung tissue: Maximum concentrations of levofloxacin in lung tissues after oral administration of 500 mg were approximately 11.3 μg/g and were achieved in 4-6 hours after drug use. The concentration in lungs exceeds the one in blood plasma.
Penetration into bladder content: Maximum concentrations of levofloxacin 4.0-6.7 μg/mL in bladder content were achieved in 2-4 hours after drug administration in 3 days of drug use at doses of 500 mg once or twice a day respectively.
Penetration into cerebrospinal liquid: Levofloxacin penetrates badly into cerebrospinal liquid.
Penetration into prostate tissues: After use of 500 mg of levofloxacin once a day during 3 days, mean concentrations in prostate tissues achieved 8.7 μg/g, 8.2 μg/g and 2.0 μg/g respectively in 2 hours, 6 hours and 24 hours; mean concentration ratio prostate/plasma was 1.84.
Urine concentration: Mean urine concentrations in 8-12 hours after single administration of oral dose 150 mg, 300 mg or 500 mg of levofloxacin were 44 mg/l, 91 mg/l and 200 mg/l respectively.
Biotransformation: Levofloxacin is poorly metabolized, metabolites are desmethyl-levofloxacin and levofloxacin N-oxide.
These metabolites cover less than 5% of drug quantity, eliminated with urine. Levofloxacin is stereochemically stable and is not entitled to inversion of chiral structure.
Elimination: After oral and intravenous administration, levofloxacin is eliminated from blood plasma rather slowly (half-life is 6-8 hours). Generally, it is eliminated by kidneys (over 85% of administered dose).
There is no significant difference regarding pharmacokinetics of levofloxacin after intravenous and oral administration, showing that these routes (oral and intravenous) are interchangeable.
Linearity: Levofloxacin follows linear pharmacokinetics in a range of 50-600 mg.
Patients with renal insufficiency: Renal insufficiency has effect on pharmacokinetics of levofloxacin. In case of nephratonia, renal elimination and clearance is decreased, and half-life periods are increased as it is shown in the table as follows: See Table 4.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageElderly patients: There are no significant differences in pharmacokinetics of levofloxacin in young patients and elderly patients, except for differences related to creatinine clearance.
Gender differences: Separate analysis regarding female and male patients showed insignificant differences in pharmacokinetics of levofloxacin depending on sex. There is no evidence of the fact that these gender differences are clinically significant.