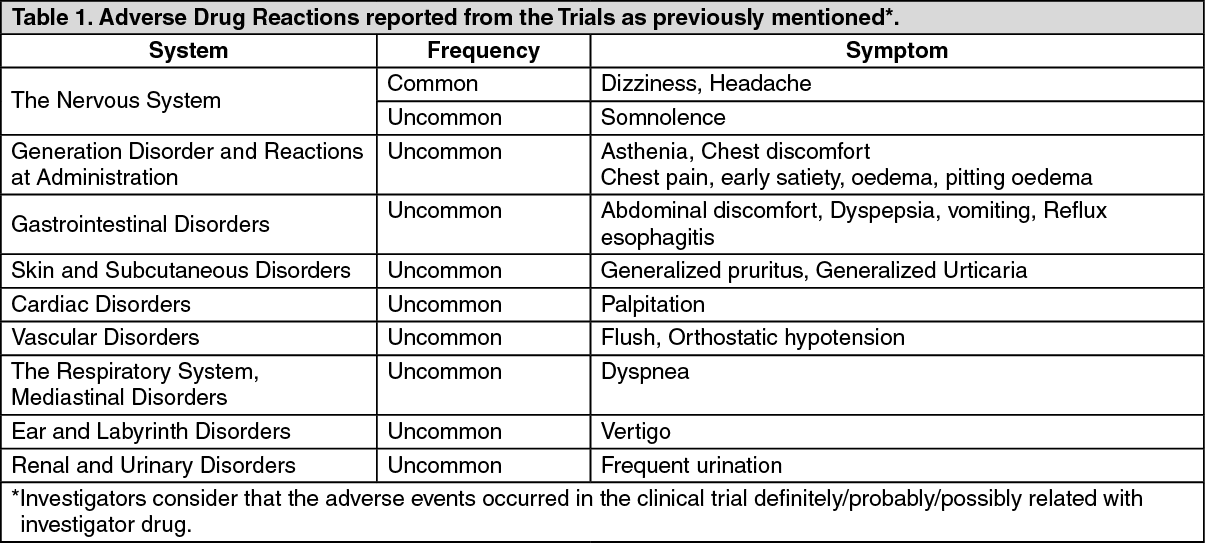
The safety of FAVOTAN has been evaluated in three controlled clinical studies with 646 patients with essential hypertension, 325 of whom received amlodipine/losartan in combination during weeks (Trial 201, 301 and 302). Adverse reactions have been ranked under headings of frequency using the following convention: Very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1,000, <1/100); rare (≥1/10,000, <1/1,000); very rare (<1/10,000). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional Safety Information from single active ingredient: Adverse drug reactions previously reported with individual components (amlodipine or losartan) may occur while taking the drug, even if not observed in clinical trials of this product.
Amlodipine: In general, treatment with amlodipine was well-tolerated. In placebo-controlled clinical trials with hypertension patients and/or angina pectoris patients, most frequently reported adverse events which are not included as previously mentioned are as follows:
General system: fatigue.
Cardiovascular system: oedema.
Gastrointestinal system: abdominal pain.
No abnormal findings on laboratory test with clinical significance in the clinical trials associated with amlodipine were reported.
Following adverse events were reported with relatively low frequency during the post-marketing period:
Autonomic Nervous System: mouth dryness, hyperhidrosis.
General: asthenia, back pain, malaise, pain, weight gain, weight decrease.
Cardiovascular: hypotension, syncope.
Central and Peripheral Nervous system: hypertonia, hyperesthesia/paresthesia, neuropathy peripheral, tremor.
Endocrine system: gynecomastia.
Gastrointestinal: change in bowel habit, gastritis, gingival hyperplasia, pancreatitis, vomiting.
Metabolic and Nutritional: hyperglycemia.
Musculoskeletal System: arthralgia, muscle cramps, myalgia.
Hemopoietic: purpura, thrombocytopenia.
Psychiatric: impotence, insomnia, dysthymic disorder.
Respiratory System: cough, dyspnea, rhinitis.
Skin and Appendages: alopecia, dyschromia, urticaria.
Special senses: dysgeusia, tinnitus.
Urinary System: micturition frequency, micturition disorder, nocturia.
Vascular system: vasculitis.
Vision: vision disorder.
Leukocytes/R.E.S: neutropenia.
Allergic reactions including pruritus, rash, angioedema, pleomorphism, erythema, hepatitis, jaundice, and hepatic enzymes elevations have been rarely reported, and most of them were related to cholestasis. For some cases, severe enough to require hospitalization have been reported in association with the use of amlodipine. The relationship of most of the events with amlodipine, however, is not certain.
Like other calcium channel inhibitors, adverse reactions as follows have been rarely reported. Whether they came from underlying disease or medication, however, could not be determined: myocardial infarction, arrhythmia (including bradycardia, ventricular tachycardia, atrial fibrillation), and chest pain.
Other reactions as follows have been reported from the use of amlodipine:
Cardiovascular system: decreased blood pressure, sinoatrial block or atrioventricular block can sometimes occur, abdominal discomfort may be rarely observed.
Gastrointestinal system: epigastric pain, diarrhea, loose stool, and constipation may sometimes occur.
Skin: erythralgia, maculopapular rash may rarely occur.
Others: sometimes pisometacarpeum, burning sensation, glucose tolerance disorder, weakness.
Losartan: The following adverse events were also reported at a rate of 1% or greater in patients treated with losartan under clinical trial with losartan monotherapy for adult patients with essential hypertension: muscle cramp, back pain, melosalgia, nasal congestion, upper respiratory infection, sinusitis, diarrhea, cough, sinus disorder, pharyngitis, myalgia, insomnia, fatigue, edema, swelling, and abdominal pain. A patient with known hypersensitivity to aspirin and penicillin, when treated with losartan, was withdrawn from study due to angioedema (swelling of the lips and eyelids and facial rash) which returned to normal 5 days after therapy was discontinued.
Superficial peeling of palms and hemolysis were reported in one subject who has received losartan. In addition to the adverse events mentioned previously, potentially significant adverse events occurred during the clinical monotherapy of losartan (<1% of patients or more than two patients) are listed as follows. It has not been determined whether these events were related to the drug:
General system: facial edema, fever, orthostatic effects, syncope.
Cardiovascular system: angina pectoris, second degree AV block, CVA, hypotension, myocardial infarction, arrhythmias including atrial fibrillation, sinus bradycardia, tachycardia, ventricular tachycardia, and ventricular fibrillation.
Gastrointestinal system: anorexia, constipation, dental pain, dry mouth, gastritis, vomiting.
Hematologic system: anemia.
Metabolic system: gout.
Musculoskeletal system: arm pain, hip pain, joint swelling, knee pain, musculoskeletal pain, shoulder pain, stiffness, arthralgia, arthritis, fibromyalgia, muscle weakness.
Nervous System Psychiatric: anxiety, anxiety disorder, ataxia, confusion, depression, nightmare, hypoesthesia, decreased sexual desire, memory impairment, migraine, nervousness, paresthesia, peripheral neuropathy, panic disorder, sleep disorder, tremor.
Respiratory System: bronchitis, pharyngeal discomfort, epistaxis, rhinitis, respiratory congestion.
Skin: alopecia, dermatitis, dry skin, ecchymosis, erythema, photosensitivity, pruritus, rash, sweating, urticaria.
Special senses: blurred vision, burning/stinging in the eye, conjunctivitis, taste perversion, tinnitus, decrease in visual acuity.
Urinary System: Impotence, nocturia, urinary tract infection.
Persistent dry cough associated with ACE-inhibitor use has been reported. This can be a cause of the discontinuation of ACE-inhibitor therapy. Two prospective, parallel-group, double-blind, randomized, controlled trials were conducted to assess the effects of losartan on the incidence of cough in hypertensive patients who had experienced cough while receiving ACE-inhibitor therapy. Patients who had typical ACE-inhibitor cough when challenged with lisinopril, whose cough disappeared on placebo, were randomized to losartan 50 mg, lisinopril 20 mg, or either placebo (n=97) or hydrochlorothiazide (n=135). The double-blind treatment period lasted up to 8 weeks. The incidence of cough is shown as follows: (See Table 2.)
Click on icon to see table/diagram/image
The studies have demonstrated that the recurrence of cough associated with losartan therapy, among patients coughed after taking ACE-inhibitor therapy, is similar to that associated with hydrochlorothiazide or placebo treatment. Cases of cough, including positive re-challenges, have been reported with the use of losartan in post-marketing experience.
The following additional adverse reactions have been reported in post-marketing experience:
Hypersensitivity: angioedema (swelling of the larynx and glottis that can cause airway obstruction, swelling of the lace/lips/pharynx/tongue) has been rarely reported in patients treated with losartan; some of these patients have previously experienced angioedema with other drugs including ACE inhibitors as well. Vasculitis (Henoch-Schonlein purpura) and anaphylactic reactions have once been reported.
Digestive: Hepatitis (reported rarely), hepatic dysfunction.
General disorder and Administration Site Conditions: malaise.
Hematologic system: anemia, thrombocytopenia (rarely reported).
Musculoskeletal system: rare cases of rhabdomyolysis have been reported in patients receiving angiotensin II receptor blockers.
Nervous system disorder: dysgeusia.
Respiratory: dry cough.
Skin: erythroderma.
Metabolic and Nutrition: hyperkalemia, hyponatremia have been reported in patients who have received losartan alone.
ALT elevations occurred rarely, but disappeared with the discontinuation of treatment.
In controlled clinical trials, clinically important changes in standard laboratory parameters were rarely associated with administration of losartan.
Creatinine, Blood Urea Nitrogen: Minor increases in blood urea nitrogen (BUN) or serum creatinine were observed in less than 0.1 percent of patients with essential hypertension treated with losartan.
Hemoglobin and Hematocrit: Small decreases in hemoglobin and hematocrit (approximately 0.11 grams percent and 0.09 volume percent, respectively) occurred in patients treated with losartan alone, but were rarely of clinical importance. No patients were discontinued the treatment due to anemia.
Liver Function Tests: Occasional elevations of liver enzymes or serum bilirubin have occurred. One patient (<0.1%) discontinued due to abnormal liver function among patients with essential hypertension treated with losartan alone.
Syncope, Apsychia: Transient symptomatic shock associated with hypotension can be occurring. Treatment should be discontinued and proper actions should be taken with the onset of related symptoms.
Acute hepatitis or fulminant hepatitis can be occurring. Treatment should be discontinued and proper actions should be taken with the onset of related symptoms.
Anaphylactic reaction.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out