Dosage of Imipenem and Cilastatin sodium is generally expressed in terms of the Imipenem content of fixed combination.
Prior to initiation Therapy with
SIANEM IV INJECTION, appropriate specimens should be obtained for identification of causative organism and in vitro susceptibility tests.
The dosage of Imipenem should be given in equally divided doses based on type and severity of infection, susceptibility of the causative organism(s), and the patient's age, body weight and renal function.
SIANEM IV INJECTION is administered by Intravenous infusion (IV infusion).
Preparation of SIANEM IV INJECTION solution for Intravenous infusion (IV infusion): Aseptic technique must be used to prepare the IV solution.
1. Reconstitute
SIANEM IV INJECTION powder in the vial with 10 mL of compatible IV solution (Compatible IV solutions are as the following: 0.9% sodium chloride injection, 5% dextrose injection, 10% dextrose injection, 5% dextrose and 0.9% sodium chloride injection, 5% dextrose and 0.45% sodium chloride injection, 5% dextrose and 0.225% sodium chloride injection, 5% dextrose and 0.15% potassium chloride injection, 5% mannitol, 10% mannitol etc.) to make an initial suspension. The resulting of initial turbid white suspension should be shaken well and then transferred to the 100-mL container of IV solution. The admixture should be agitated until it is clear to yield 5 mg/mL of Imipenem.
Note: The initial reconstituted suspension is not for direct infusion.
2.
Aseptic technique must be used to reduce the risk of contamination during reconstitution.
Discard the unused portion of the IV infusion solution.
3. Color of solution of
SIANEM IV INJECTION ranges from clear and colorless to pale yellow. Variations of color within this range do not affect potency.
4.
SIANEM IV INJECTION should be inspected visually for particulate matter or discoloration prior to administration.
Note:
SIANEM IV INJECTION should not be prepared with IV infusion solution containing lactate.
Do not mix with other antimicrobial.
Solution of
SIANEM IV INJECTION must be clear before administration.
Do not use when the Solution of
SIANEM IV INJECTION is in turbid white suspension.
Agitation of admixture may result in the visible air bubbles while reconstituted solution which do not affect the potency.
Should not be heated to dissolution.
Stability: After reconstituted
SIANEM IV INJECTION is stable for 4 hours at room temperature (25°C). Thus it is recommended to use the solution within the first hour after reconstituted. The reconstituted solution is stable for 24 hours if refrigerated at 2-8°C (do not freeze).
Discard the remaining after the mixture.
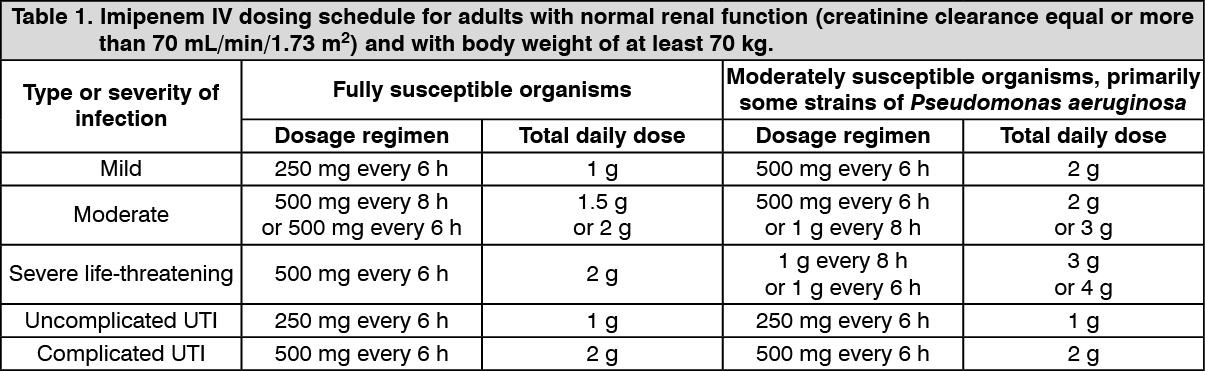
Dosage: Adult dosage: The dosage depends on the type and severity of the infections (see Table 1).
The maximum recommended IV dosage of Imipenem for adult is 50 mg/kg daily or 4 g daily, whichever is lower. The rate of IV infusion of Imipenem should generally be infused over 20-30 minutes.
However, patients who have received more than 500 mg dose of Imipenem should be infused over 40-60 minutes. If nausea and/or vomiting occur during administration of Imipenem, the rate of IV infusion should be decreased. (See Table 1.)
 Click on icon to see table/diagram/image
Note:
Click on icon to see table/diagram/image
Note: For surgical infection prophylaxis in adults, Imipenem 1 g may be given intravenously on induction of anesthesia, followed by a further 1 g three hours later, with additional 500 mg twice with 8 hours interval after induction if necessary.
For patients older than 12 years of age with cystic fibrosis and normal renal function, Imipenem may be given daily dosage up to 90 mg/kg (maximum daily dosage: 4 g), in divided doses.
Children dosage: Non CNS-infections dosage 15 to 25 mg/kg/dose IV every 6 hours but the maximum recommended IV dosage of Imipenem for children is 2 g daily in those with infections caused by fully susceptible bacteria or 4 g daily in those with infections caused by moderately susceptible bacteria (e.g. some strains of
Pseudomonas aeruginosa).
When IV Imipenem and Cilastatin sodium is used in children, dose of 500 mg or less should be given by IV infusion over 15-30 minutes and doses greater than 500 mg should be given by IV infusion over 40-60 minutes.
Children dosage of Imipenem should be given in equally divided doses based on the patient's age and body weight.
3 months of age or older: 15-25 mg/kg every 6 hours.
4 weeks to 3 months of age and weight at least 1.5 kg: 25 mg/kg every 6 hours.
1 to 4 weeks of age and weight at least 1.5 kg: 25 mg/kg every 8 hours.
Up to 1 week of age and weight at least 1.5 kg: 25 mg/kg every 12 hours.
Note: 1.
SIANEM IV INJECTION should not be used in children with CNS infections, due to risk of seizure.
2.
SIANEM IV INJECTION should not be use in children with impaired renal function who have weight less than 30 kg because of insufficient safety data.
Dosage in renal function impairment: Adult dosage: Adult IV dosage of Imipenem should be reduced in patients with renal impairment based on the patient's creatinine clearance and body weight. (See Table 2.)
Click on icon to see table/diagram/image
Hemodialysis: Imipenem and Cilastatin sodium is cleared by hemodialysis. Doses should be given after hemodialysis and at 12-hour intervals time from the end of that dialysis session.
For patients on hemodialysis, Imipenem and Cilastatin sodium is recommended only when the benefits outweigh the potential risk of seizures and other CNS symptom. Carefully monitor dialysis patients.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image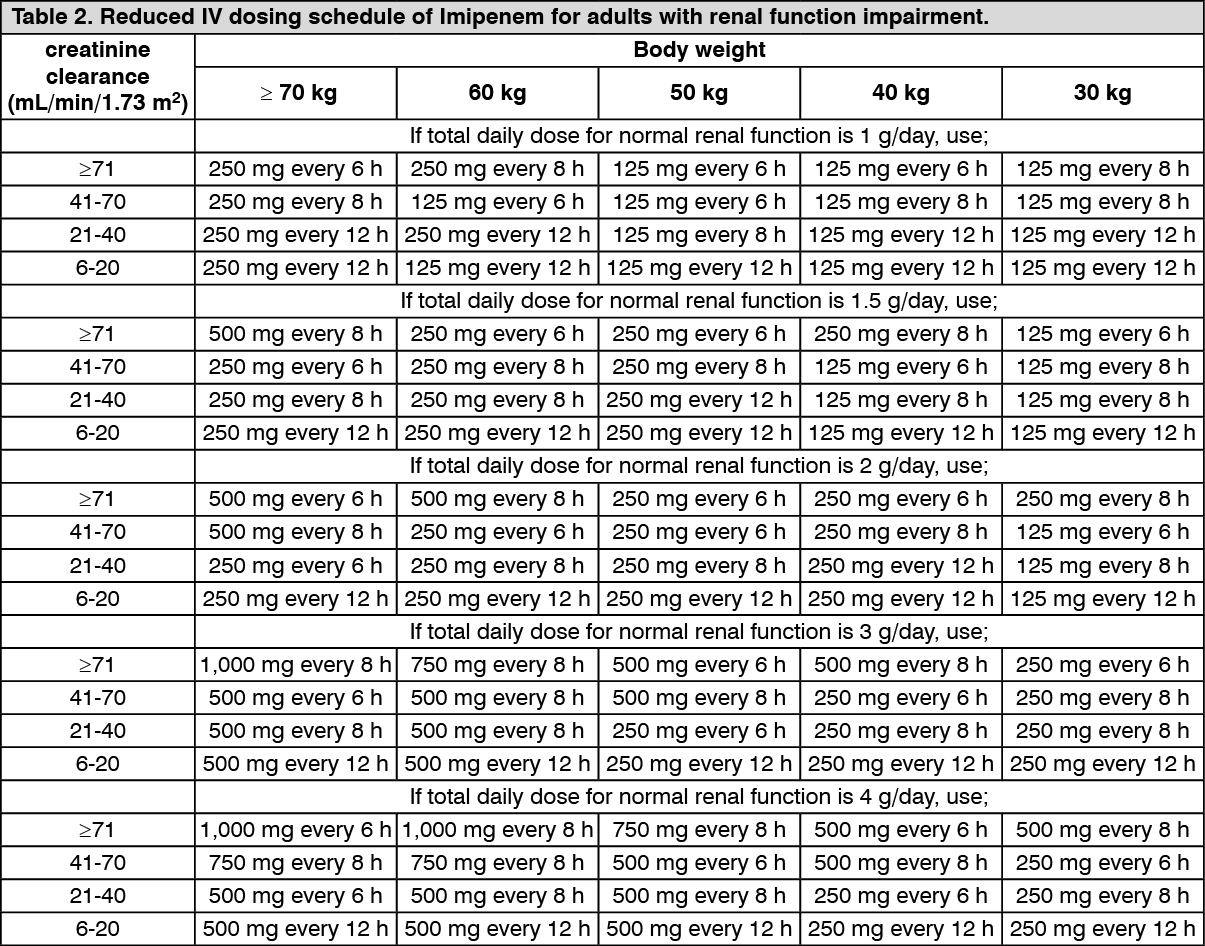 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out