Film-coated extended-release tablets based on the hydrophilic gel matrix principle.
The Plendil 2.5 mg tablet is yellow, circular, biconvex, engraved A/FL on one side and 2.5 on the other side, with a diameter of 8.5 mm.
The Plendil 5 mg tablet is pink, circular, biconvex, engraved A/Fm on one side and 5 on the other side, with a diameter of 9 mm.
The Plendil 10 mg tablet is reddish-brown, circular, biconvex, engraved A/FE on one side and 10 on the other side, with a diameter of 9 mm.
Excipients/Inactive Ingredients: Carnauba wax, hydroxypropylcellulose, hydroxypropyl methylcellulose, iron oxides E 172, lactose anhydrous, microcrystalline cellulose, polyethylene glycol 6000, polyoxyl 40 hydrogenated castor oil, propyl gallate, sodium aluminium silicate, sodium stearyl fumarate, titanium dioxide E 171, water purified.
Pharmacotherapeutic group: Calcium antagonist. ATC Code: C08CA02.
Pharmacology: Pharmacodynamics: Felodipine (Plendil) is a vasoselective calcium antagonist for the treatment of hypertension and stable angina pectoris.
The active substance in Plendil, felodipine, is a dihydropyridine derivate. Felodipine is a racemate. Felodipine exerts its effect by reducing peripheral vascular resistance, particularly in arterial resistance vessels. The electrical and contractile activity of vascular smooth muscle cells is inhibited via an effect on the calcium channels in the cell membranes.
Due to the selective effect on smooth muscle in arterial resistance vessels, felodipine in therapeutic doses has no negative inotropic effects on the heart, nor any clinically significant electrophysiological cardiac effects. Felodipine relaxes smooth muscle in the airways. Clinical experience has shown that felodipine has little effect on gastrointestinal muscle motor function. No clinically significant effect of felodipine on blood lipids has been observed during long-term treatment, nor have any clinically significant effects on metabolic control (HbA1c) been observed in patients with type II diabetes during six months of treatment.
Felodipine can generally also be given to patients with concomitant impairment of left ventricular function who receive conventional therapy, or with asthma, diabetes mellitus, gout or hyperlipidaemia.
Anti-hypertensive effect: Felodipine lowers arterial blood pressure by decreasing peripheral vascular resistance. Treatment of hypertensive patients with Plendil reduces the blood pressure, both in the sitting and standing position and at rest and during exercise. Felodipine does not give rise to orthostatic hypotension, as the substance has no effect on venous smooth muscle or adrenergic control mechanisms.
The lowered blood pressure may initially cause a temporary reflex increase in heart rate and cardiac output. The increased heart rate is counteracted when felodipine is given together with β-blockers. Plasma concentrations of felodipine are positively correlated to the decrease in total peripheral resistance and blood pressure. At steady state the effect remains over the entire dose range and gives a 24-hour reduction in blood pressure.
Treatment with felodipine is associated with regression of left ventricular hypertrophy.
Felodipine has a natriuretic and diuretic effect but no potassiuretic effect. The tubular reabsorption of sodium and water is reduced, which may explain the absence of salt and fluid retention in the patient. Felodipine reduces renal vascular resistance and increases renal perfusion. The glomerular filtration rate is unchanged. Felodipine does not influence urinary albumin excretion.
In the so-called HOT (Hypertension Optimal Treatment) study, including 18,790 patients with mild to moderate hypertension, treatment with Plendil, in combination with an angiotensin-converting enzyme (ACE) inhibitor, a β-blocker and/or a diuretic, if needed, resulted in a diastolic blood pressure (DBP) of ≤ 90 mmHg in 93% of the patients.
In the same study, the incidence of cardiovascular events in patients with type II diabetes (n=1501) was significantly lower (50%) in the group where the target DBP was ≤ 80 mmHg (11.9/1000 patient years), compared with the group where the target DBP was below 90 mmHg (24.4/1000 patient years).
Plendil was included as one of two calcium antagonists in the Swedish STOP-2 study, performed in 6,614 patients aged 70-84 years. The study indicates that hypertensive treatment initiated with dihydropyridine calcium antagonists and with the addition of β-blockers, if needed, has no effect of cardiovascular mortality compared with conventional treatment with β-blockers and/or diuretics.
For the treatment of hypertensive patients, Plendil can be used as monotherapy or in combination with other antihypertensive drugs, such as β-blockers, diuretics or ACE inhibitors.
Anti-anginal effect: Felodipine exerts its effect through dilatation of coronary vessels, which also improves perfusion and the oxygen supply to the heart. Cardiac workload is decreased through a reduction of the peripheral arterial resistance (reduced afterload), which results in reduced oxygen demand in the myocardium. Coronary vasospasm is counteracted by felodipine.
Felodipine improves exercise capacity and reduces anginal attacks in patients with stable effort-induced angina pectoris.
Initially during treatment there is a transient reflex increase in heart rate, which is counteracted if Plendil is given in combination with a β-blocker. The time to onset of effect is two hours and the effect duration is 24 hours.
Felodipine can be used in combination with β-adrenoceptor blockers or as monotherapy for the treatment of patients with angina pectoris.
Pharmacokinetics: The active substance in Plendil extended-release tablets, felodipine, is imbedded in a polymer that forms a gel layer in contact with water, from which felodipine is released continuously, which leads to a slow onset of effect.
The bioavailability of felodipine is approximately 15% and is independent of concomitant food intake. However, the rate of absorption, although not the degree of absorption, is affected by concomitant intake of food, and the maximum plasma concentration is thereby increased by approximately 65%. The maximum plasma concentration is reached after 3-5 hours. The degree of binding to plasma proteins is approximately 99%. The distribution volume at steady state is 10 L/kg. The half-life of felodipine in the elimination phase is approximately 25 hours and steady state is reached after 5 days. There is no risk of accumulation during long-term treatment.
Average clearance is 1200 ml/min. Reduced clearance in elderly patients and patients with impaired liver function leads to higher plasma concentrations of felodipine. However, age can only partly explain the interindividual variations in plasma concentrations. Felodipine is metabolised in the liver and none of the identified metabolites has a vasodilating effect. About 70% of a given dose is excreted as metabolites in the urine and the rest is excreted in the faeces. Less than 0.5% of a given dose is recovered unchanged in the urine.
Impaired renal function does not affect plasma concentrations of felodipine, although there is accumulation of inactive metabolites. Felodipine is not eliminated by haemodialysis.
Hypertension. Stable angina pectoris.
The tablets should be taken in the morning, be swallowed with water and must not be divided, chewed or crushed. The tablets can be administered without food or following a light meal not rich in fat or carbohydrates.
Hypertension: The dose should be adjusted individually. Treatment should be initiated with 5 mg once daily. If necessary, the dose may be further increased or another antihypertensive agent added. The usual maintenance doses are 5 mg to 10 mg once daily.
Stable angina pectoris: The dose should be adjusted individually. Treatment should be started with 5 mg once daily, increasing to 10 mg once daily if needed.
Elderly patients: In elderly patients initial treatment with 2.5 mg daily should be considered.
Impaired renal function: Impaired renal function does not affect plasma concentrations of felodipine. No dose adjustment is required. However, Plendil should be used with caution in patients with severely impaired renal function (see Pharmacology: Pharmacokinetics under Actions).
Impaired hepatic function: Patients with impaired hepatic function may have elevated plasma concentrations of felodipine and may respond to treatment at lower doses.
Paediatric population: Felodipine should, due to limited clinical trial experience, not be used in pediatric patients.
Toxicity: 10 mg to a two-year-old child caused mild intoxication. 150-200 mg to a 17-year-old and 250 mg to an adult caused mild to moderate intoxication. Felodipine probably has a more pronounced effect on the peripheral circulation than on the heart, compared with other drugs in the same group.
Symptoms: The symptoms of intoxication with extended-release tablets may be delayed 12-16 hours and severe symptoms may set in after several days. Circulatory effects constitute the greatest risk: bradycardia (sometimes tachycardia), AV block I-III, AV dissociation, VES, ventricular fibrillation, asystole. Dizziness, headache, impaired consciousness, coma, spasms. Dyspnoea, lung oedema (non-cardiac) and apnoea. Possibly ARDS (Adult Respiratory Distress Syndrome). Acidosis, hypokalaemia, hyperglycaemia, potentially hypocalcaemia. Flush, hypothermia. Nausea and vomiting.
Management: Activated charcoal, gastric lavage if indicated, in certain cases also late after exposure (extended-release tablets can aggregrate).
Atropine (0.25-0.5 mg intravenously to adults, 10-20 mcg/kg to children) should be given before gastric lavage (due to the risk of vagal stimulation).
ECG monitoring. Respirator treatment on broad indication. Correction of acid-base and electrolyte status.
If severe hypotension occurs, symptomatic treatment should be initiated. The patient should be placed in a supine position with the legs elevated. In the event of accompanying bradycardia, 0.5-1.0 mg atropine should be administered intravenously. If this is not sufficient, plasma volume should be increased by infusion of e.g. glucose, saline or dextran. Sympathomimetics with predominant effect on the α1-adrenoceptor may be given if the aforementioned measures are not sufficient.
In circulatory arrest, resuscitation attempts may be required during several hours. In the case of spasms, diazepam should be given. Otherwise symptomatic therapy.
Pregnancy; Known hypersensitivity to felodipine or any other component of the product (see Description); Uncompensated heart failure; Acute myocardial infarction; Unstable angina pectoris; Dynamic cardiac outflow obstruction; Haemodynamically significant cardiac valvular obstruction; Cardiogenic shock.
Felodipine can, like other vasodilators, cause hypotension. This may in susceptible patients result in myocardial ischemia.
Mild gingival enlargement has been reported in patients with pronounced gingivitis/periodontitis. The enlargement can be avoided or reversed by careful dental hygiene.
Plendil contains lactose and should not be given to patients with hereditary galactose intolerance or glucose-galactose malabsorption.
Effects on ability to drive and use machines: As dizziness and fatigue may occur in connection with Plendil treatment, this should be considered when enhanced attention is required, for example, when driving or operating machines.
Fertility: Data on male and female fertility in patients are missing.
Pregnancy: Relevant data from treatment of pregnant women with Plendil is lacking. Plendil should not be used during pregnancy, as teratogenic effects have been seen in animal studies. Calcium antagonists may inhibit premature contractions in the uterus, but there is no definite evidence of delayed delivery in a full-term pregnancy. There is a risk of development of hypoxia in the foetus in hypotensive mothers and of decreased perfusion of the uterus, due to a redistribution of the blood flow through peripheral vasodilatation.
Lactation: Felodipine is excreted in the breast milk. If the mother uses therapeutic doses of felodipine, only a very small dose is transferred via the breast milk to the child. There is insufficient experience of treatment with felodipine during lactation for an assessment of the risks to the child. For this reason, Plendil should not be given during lactation. In cases where the medical benefit of continued treatment is considered to be greater than the risk, stopping lactation should be considered.
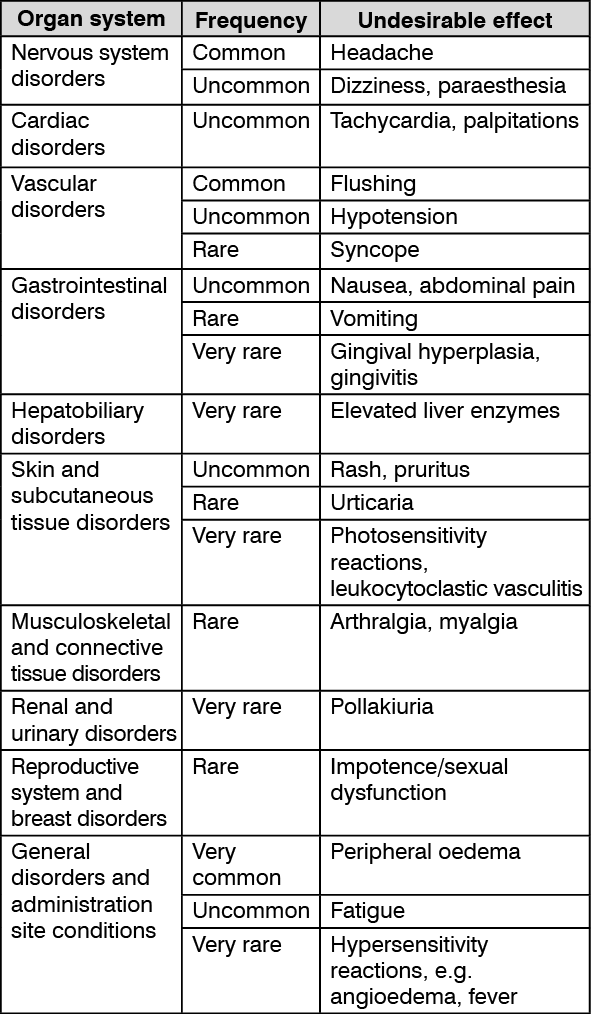
Felodipine can cause flushing, headache, palpitations, dizziness and fatigue. Most of these reactions are dose-related and appear at the start of treatment or after a dose increase. If such reactions occur, they are usually transient and abate with time.
Dose-related ankle swelling can occur in patients treated with felodipine. This results from precapillary vasodilatation and is not related to any generalised fluid retention. Experience from clinical trials has shown that 2% of patients interrupted treatment due to ankle swelling.
Occasional cases of confusion and sleep disturbances have been reported, but a connection with felodipine has not been established with certainty.
Mild gingival enlargement has been reported in patients with pronounced gingivitis/periodontitis. The enlargement can be avoided or reversed by careful dental hygiene.
Hyperglycaemia is a class-related undesirable effect, but has only been reported in individual cases for felodipine.
The following frequency definitions are used: Very common ≥1/10; Common ≥1/100, <1/10; Uncommon ≥1/1,000, <1/100; Rare ≥1/10,000, <1/1,000; Very rare <1/10,000. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Felodipine is metabolised in the liver by cytochrome P450 3A4 (CYP3A4). Concomitant administration of substances which interfere with the CYP3A4 enzyme system may affect plasma concentrations of felodipine.
CP3A4 inducers: Drugs that increase the metabolism of felodipine by induction of P450 are, for example, carbamazepine, phenytoin, phenobarbital and rifampicin, as well as St. John's wort (Hypericum perforatum). When Plendil was administered together with carbamazepine, phenytoin and phenobarbital, the AUC of felodipine was reduced by 93% and Cmax by 82%. Combination with CYP3A4 inducers should be avoided.
CYP3A4 inhibitors: Drugs that are potent CYP3A4 inhibitors are for example, azole antimycotics (itraconazole, ketoconazole), macrolide antibiotics (erythromycin) and HIV protease inhibitors. Concomitant administration of itraconazole resulted in eight-fold increases of the Cmax of felodipine and six-fold increases of the AUC. Concomitant administration of erythromycin led to approximately 2.5-fold increases of the Cmax and the AUC of felodipine. Combination with potent CYP3A4 inhibitors should be avoided.
Grapefruit juice inhibits CYP3A4. Administration of felodipine together with grapefruit juice resulted in approximately two-fold increases of the Cmax and the AUC of felodipine. Combination with grapefruit juice should be avoided.
Tacrolimus: Felodipine may increase the concentration of tacrolimus. When used together, the concentration in serum of tacrolimus should be monitored and the tacrolimus dose may need to be adjusted.
Cyclosporin: Concomitant treatment with cyclosporin and felodipine increased the plasma concentration of felodipine by 150% and the AUC by 60%. The effect of felodipine on the pharmacokinetics of cyclosporin is, however, limited.
Cimetidine: Concomitant treatment with cimetidine and felodipine increased the Cmax and AUC of felodipine by approximately 55%.
C08CA02 - felodipine ; Belongs to the class of dihydropyridine derivative selective calcium-channel blockers with mainly vascular effects. Used in the treatment of cardiovascular diseases.
Plendil XR tab 10 mg
30's
Plendil XR tab 2.5 mg
300's;30's
Plendil XR tab 5 mg
300's;30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out